The Center for Critical Care Nephrology, Department of Critical Care Medicine, University of Pittsburgh School of Medicine, Pittsburgh, PA, United States of America; The CRISMA (Clinical Research, Investigation and Systems Modeling of Acute Illness) Center, Department of Critical Care Medicine, University of Pittsburgh School of Medicine, Pittsburgh, PA, United States of America; Excellence Center for Critical Care Nephrology, Division of Nephrology, Faculty of Medicine, Chulalongkorn University, Bangkok, Thailand; Critical Care Nephrology Research Unit, Faculty of Medicine, Chulalongkorn University, Bangkok, Thailand; Department of Laboratory Medicine, Faculty of Medicine, Chulalongkorn University, Bangkok, Thailand.
The Center for Critical Care Nephrology, Department of Critical Care Medicine, University of Pittsburgh School of Medicine, Pittsburgh, PA, United States of America; The CRISMA (Clinical Research, Investigation and Systems Modeling of Acute Illness) Center, Department of Critical Care Medicine, University of Pittsburgh School of Medicine, Pittsburgh, PA, United States of America; Department of Emergency and Organ Transplantation, Nephrology, Dialysis and Transplantation Unit, University of Bari, Bari, Italy.
J Crit Care. 2023 Aug;76:154280. doi: 10.1016/j.jcrc.2023.154280. Epub 2023 Feb 26.
To examine the effect of kidney recovery on mortality, dialysis and kidney transplantation up to 15 years after AKI.
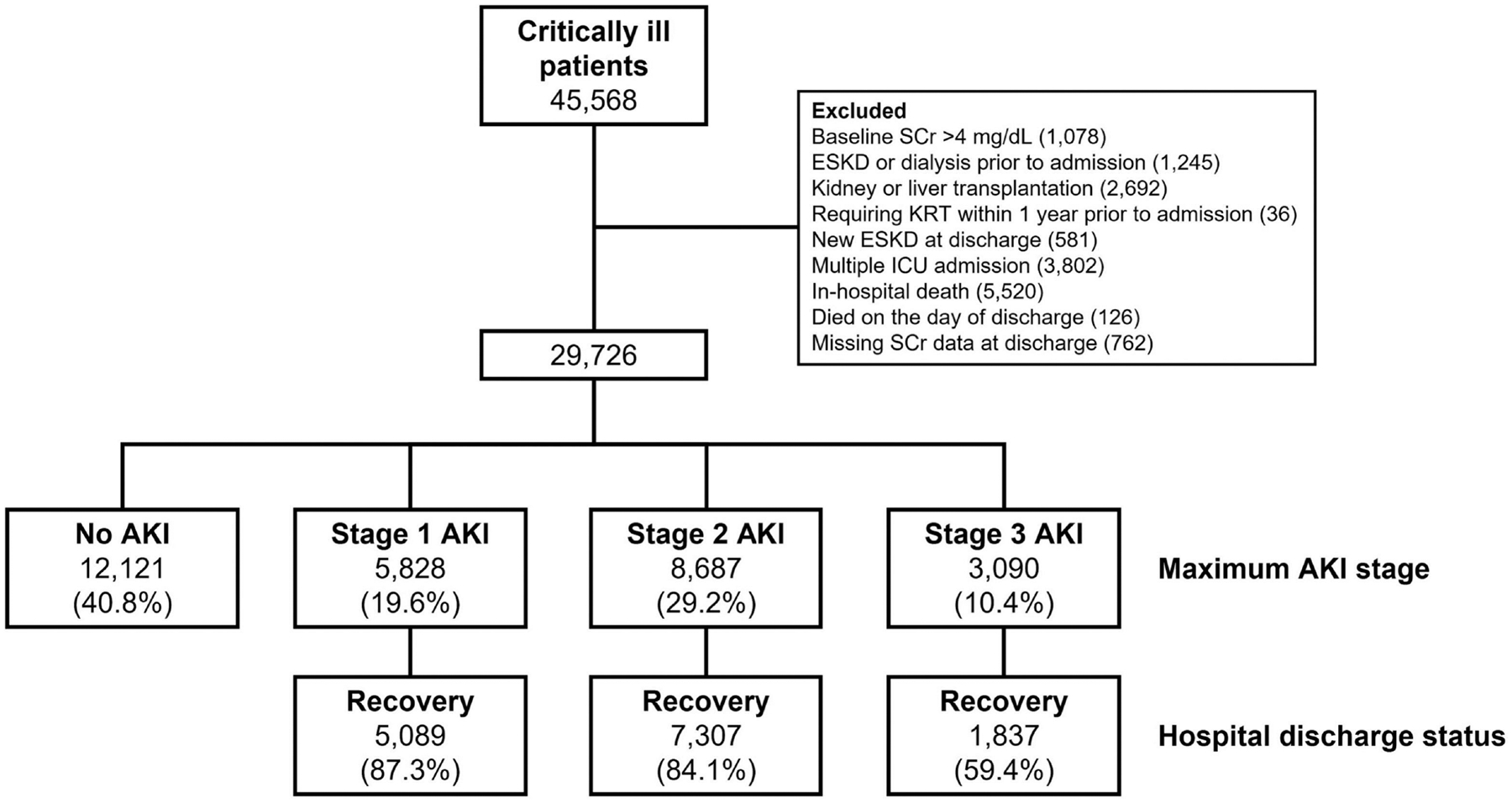
We studied 29,726 survivors of critical illness and compared these outcomes stratified by AKI and recovery status at hospital discharge. Kidney recovery was defined as a return of serum creatinine to ≤150% of baseline without dialysis prior to hospital discharge.
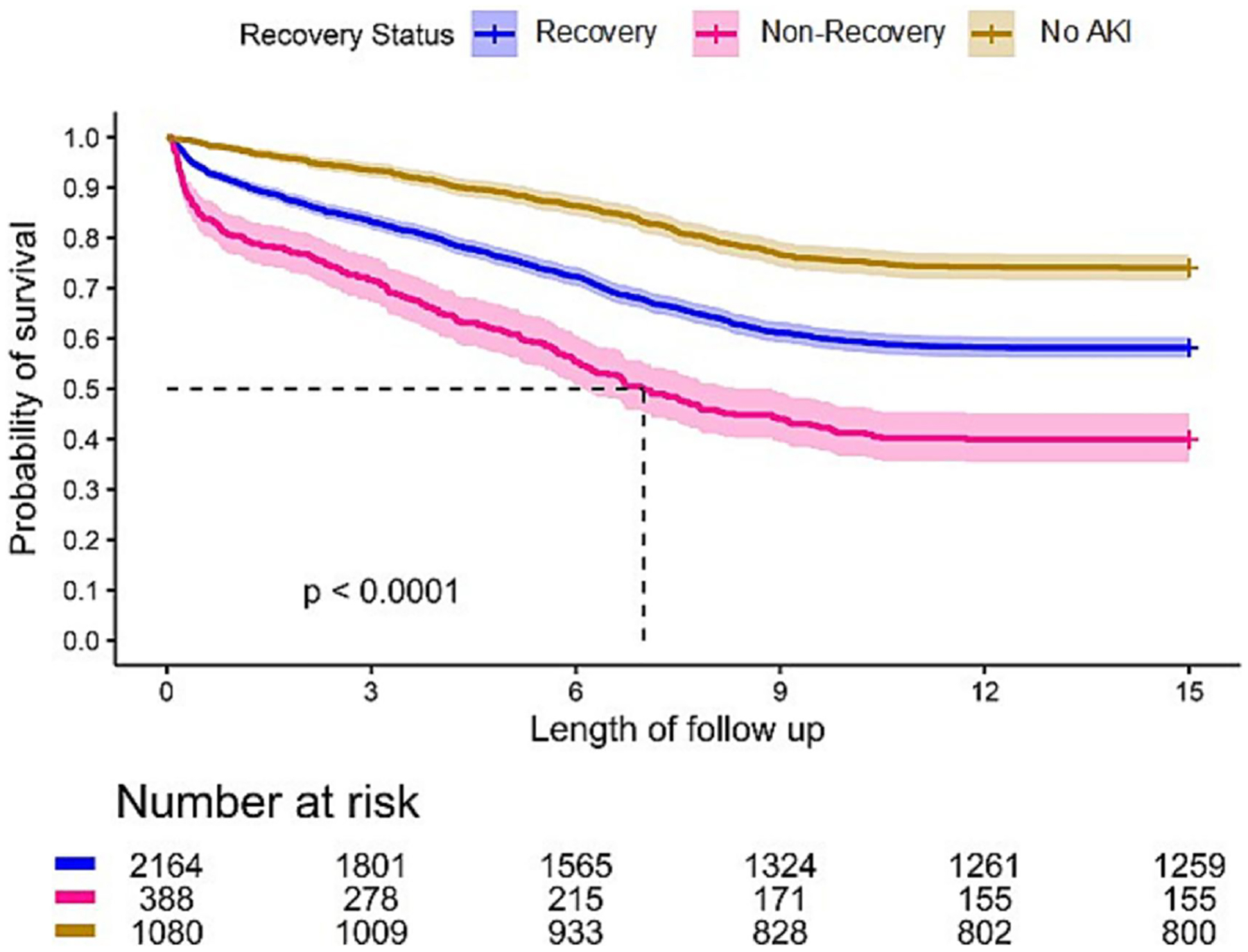
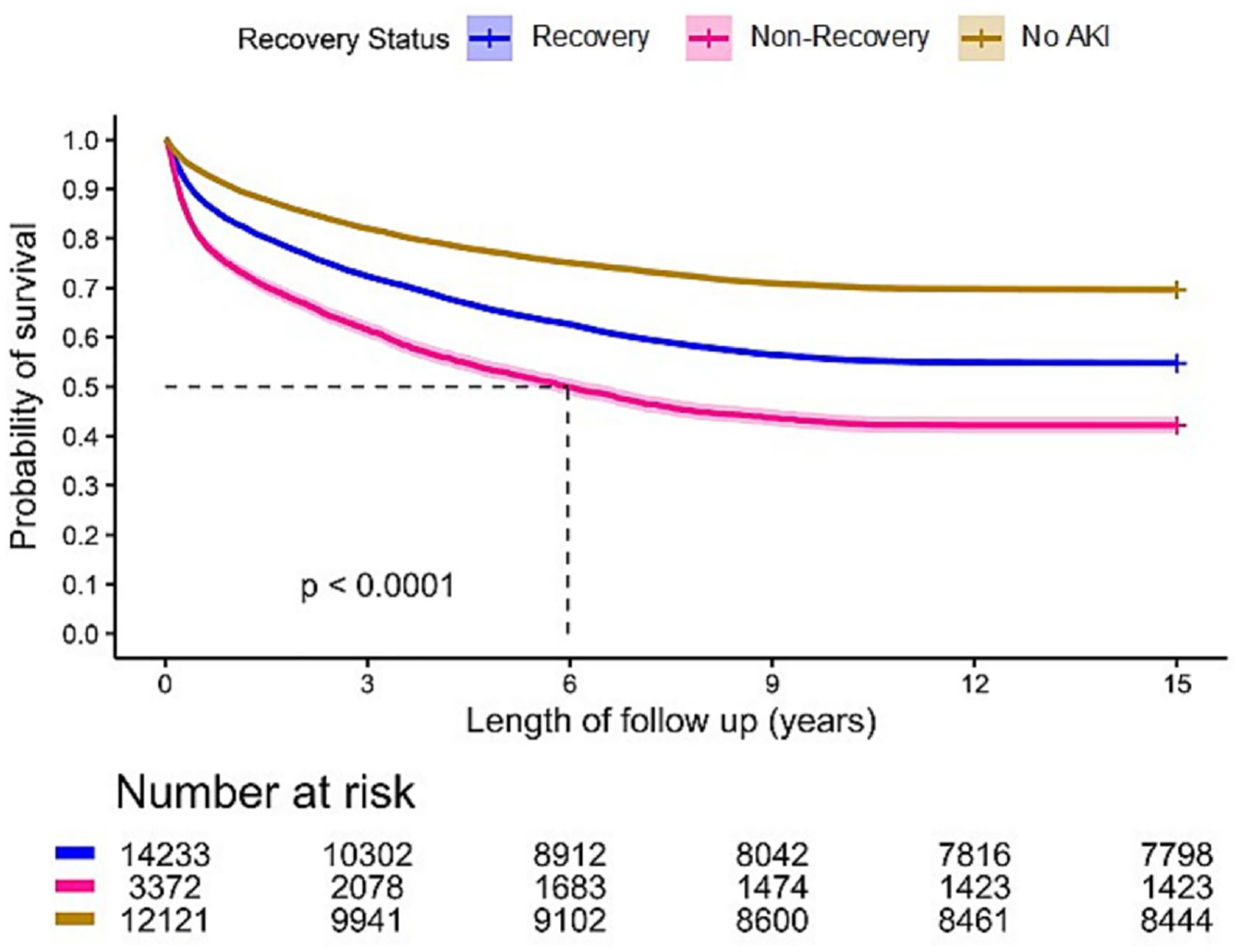
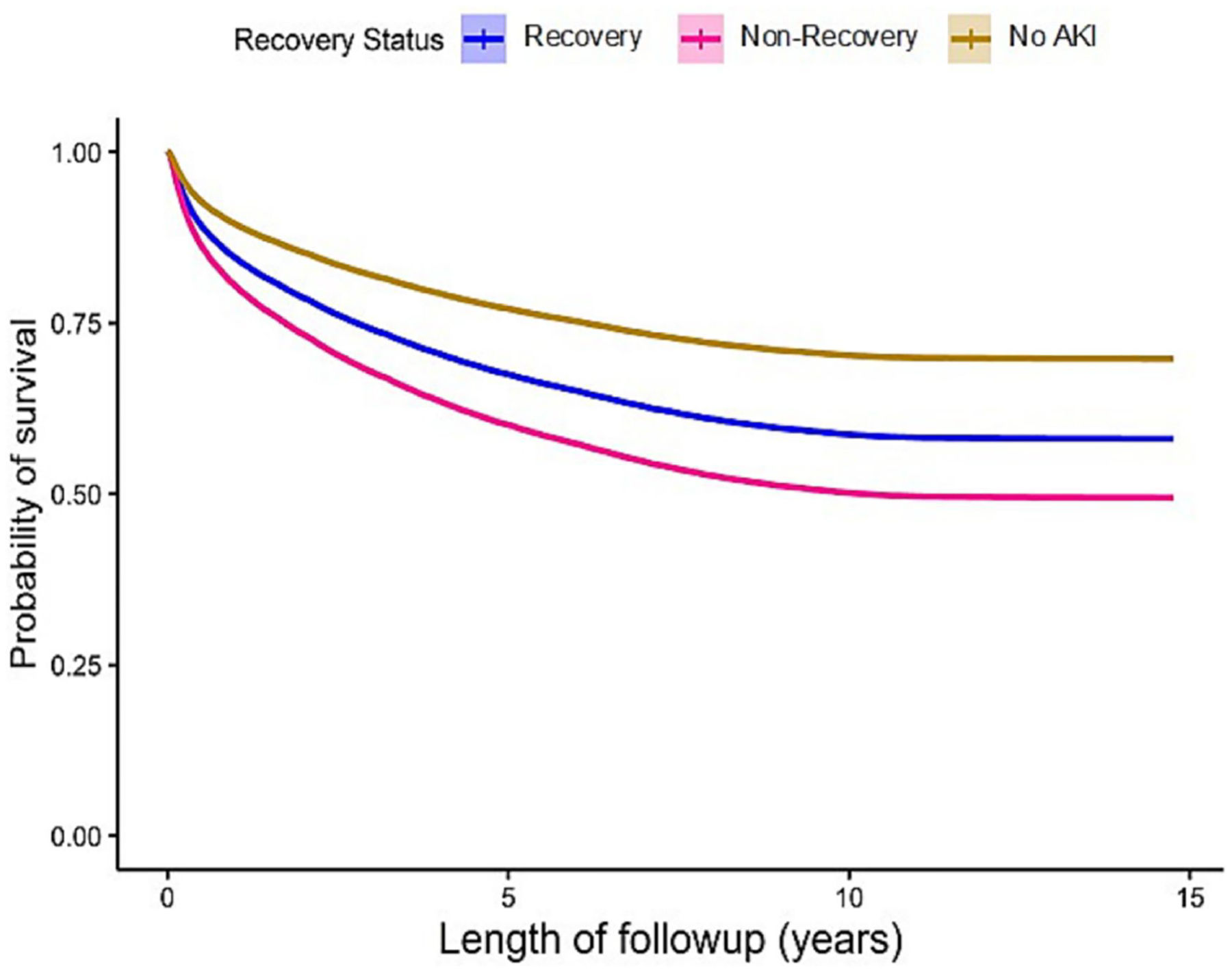
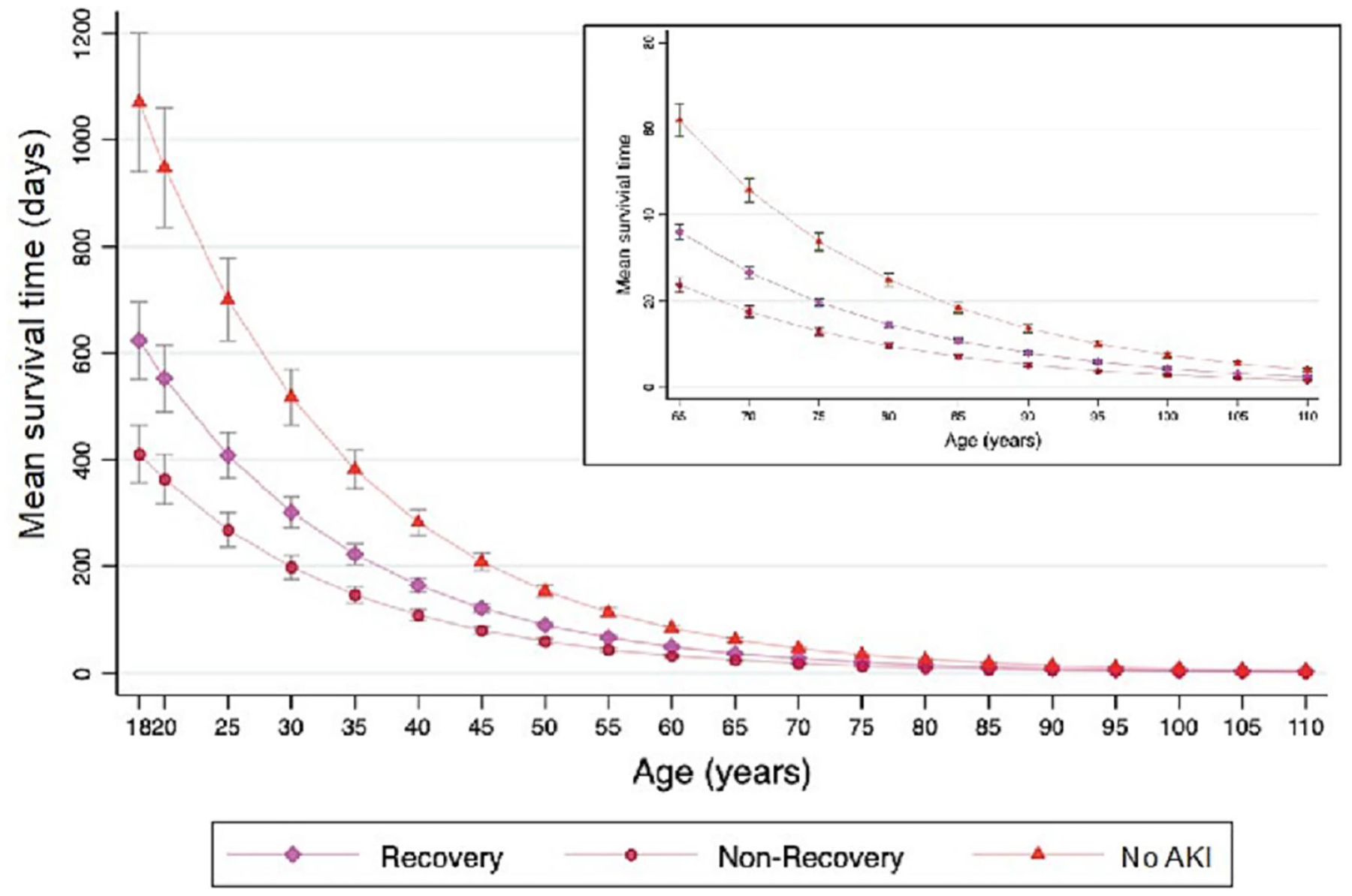
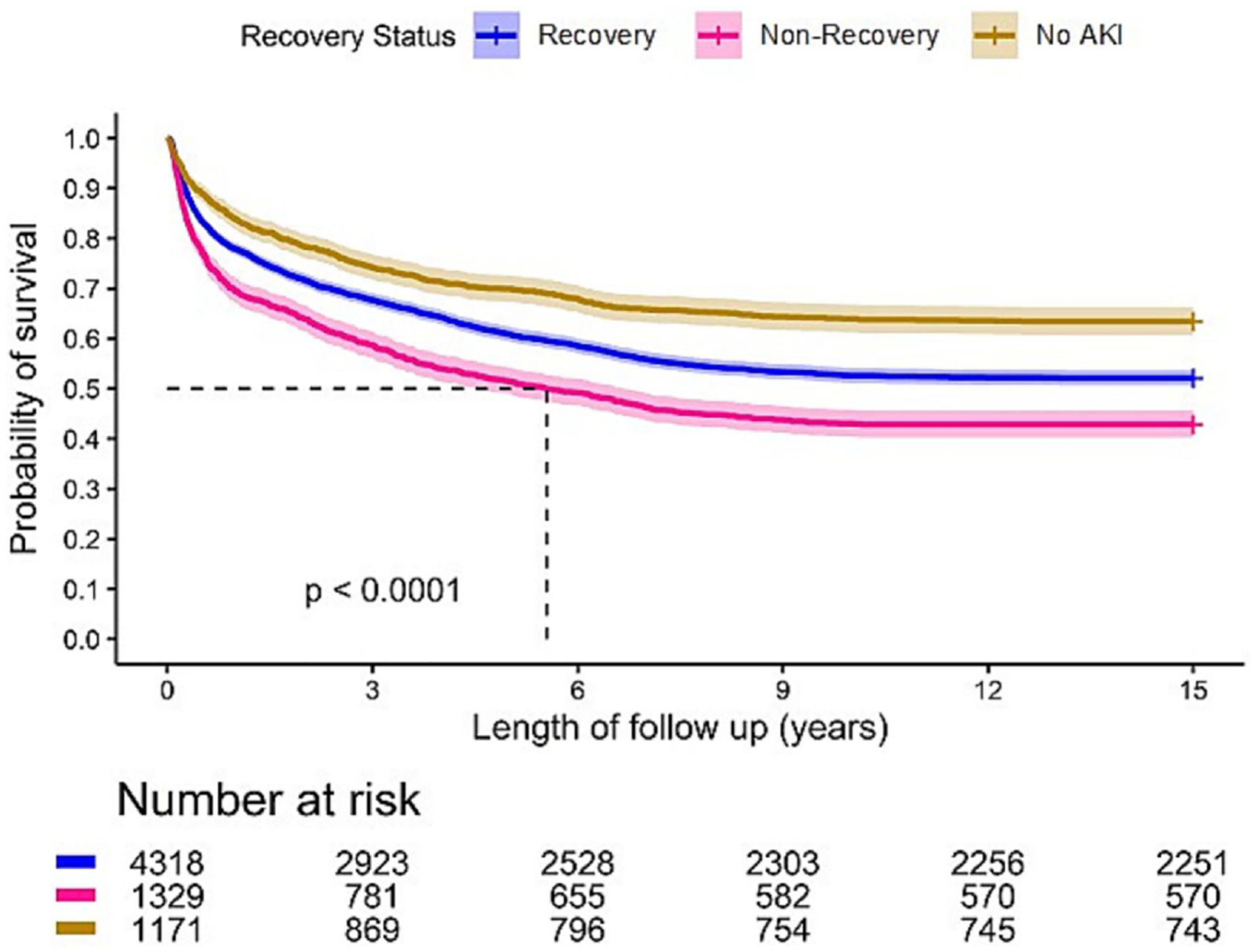
Overall AKI occurred in 59.2% in which two thirds developed stage 2-3 AKI. Recovery rate of AKI at hospital discharge was 80.8%. Patients who did not recover experienced the worst 15-year mortality compared to those who recovered and those without AKI (57.8% vs 45.2% vs 30.3%, p < 0.001). This pattern was also found in subgroups of patients with suspected sepsis-associated (57.1% vs 47.9% vs 36.5%, p < 0.001) and cardiac surgery-associated AKI (60.1% vs 41.8% vs 25.9%, p < 0.001). The rates of dialysis and transplantation at 15 years were low and not associated with recovery status.
Recovery of AKI in critically ill patients at hospital discharge had an effect on long-term mortality for up to 15 years. These results have implications for acute care, follow-up and choice of endpoints for clinical trials.
探讨急性肾损伤(AKI)后 15 年内肾功能恢复对死亡率、透析和肾移植的影响。
我们研究了 29726 例危重病幸存者,并根据 AKI 及出院时肾功能恢复情况进行分层,比较了这些结局。肾功能恢复定义为血清肌酐恢复至基线值的≤150%,且在出院前无需透析。
总体 AKI 发生率为 59.2%,其中三分之二发展为 2-3 期 AKI。出院时 AKI 的恢复率为 80.8%。与恢复的患者和无 AKI 的患者相比,未恢复的患者 15 年死亡率最高(57.8%比 45.2%比 30.3%,p<0.001)。这种模式在疑似脓毒症相关 AKI(57.1%比 47.9%比 36.5%,p<0.001)和心脏手术后相关 AKI(60.1%比 41.8%比 25.9%,p<0.001)的亚组患者中也存在。15 年时透析和移植的发生率较低,与肾功能恢复状态无关。
危重病患者出院时 AKI 的恢复对 15 年内的长期死亡率有影响。这些结果对急性护理、随访以及临床试验终点的选择具有重要意义。