Department of Human Neuroscience, Sapienza University of Rome, Rome, Italy.
Nuffield Department of Surgical Sciences, University of Oxford, John Radcliffe Oxford University Hospital, Headington, Oxford, OX3 9DU, UK.
Sci Rep. 2023 Feb 28;13(1):3400. doi: 10.1038/s41598-023-30135-8.
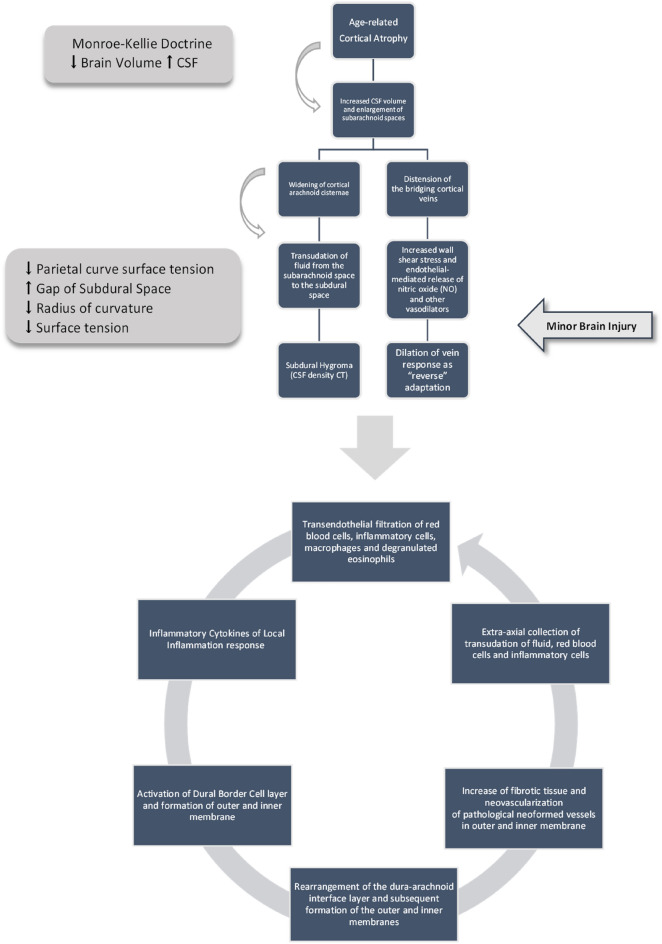
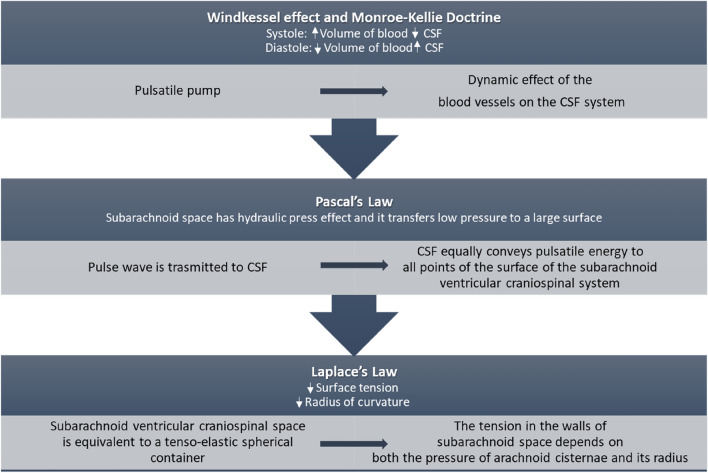
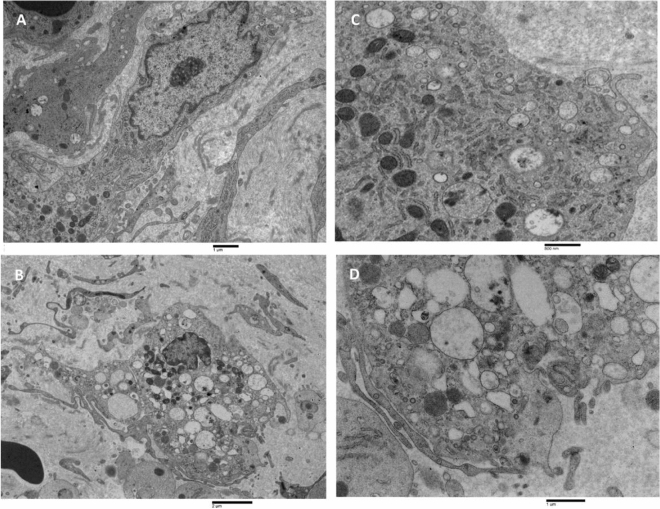
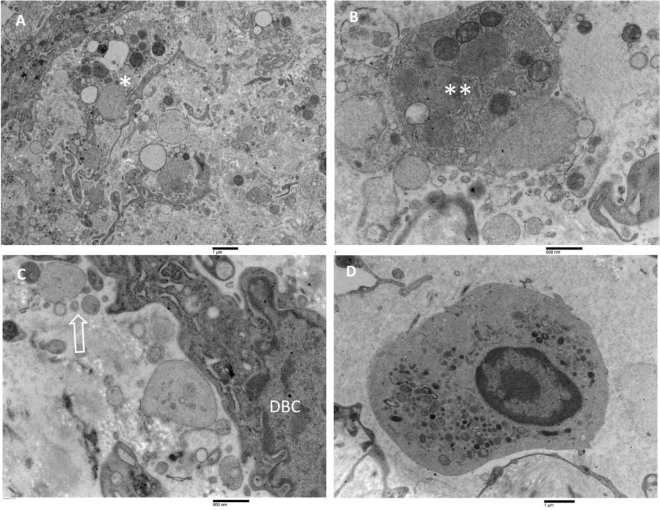
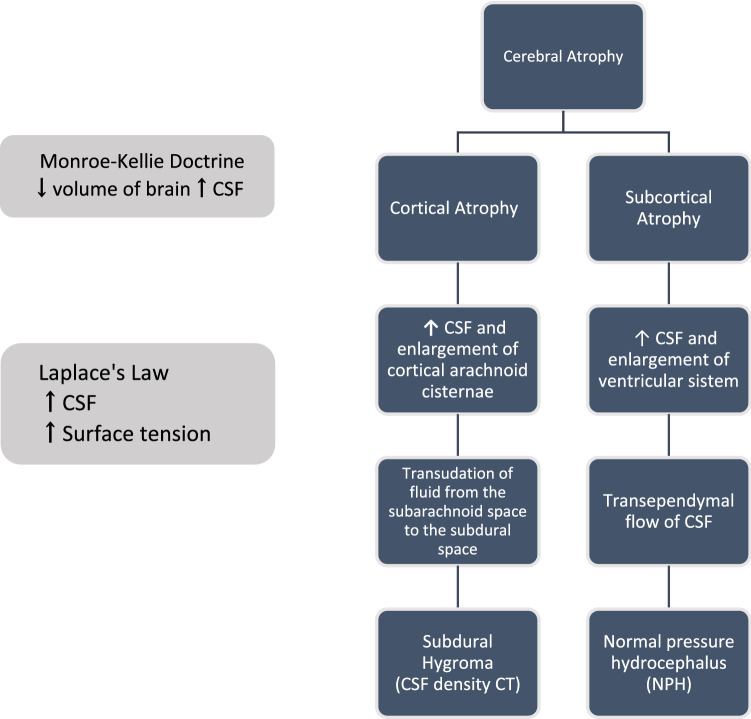
Several theories have tried to elucidate the mechanisms behind the pathophysiology of chronic subdural hematoma (CSDH). However, this process is complex and remains mostly unknown. In this study we performed a retrospective randomised analysis comparing the cortical atrophy of 190 patients with unilateral CSDH, with 190 healthy controls. To evaluate the extent of cortical atrophy, CT scan images were utilised to develop an index that is the ratio of the maximum diameter sum of 3 cisterns divided by the maximum diameter of the skull at the temporal lobe level. Also, we reported, for the first time, the ultrastructural analyses of the CSDH using a combination of immunohistochemistry methods and transmission electron microscopy techniques. Internal validation was performed to confirm the assessment of the different degrees of cortical atrophy. Relative Cortical Atrophy Index (RCA index) refers to the sum of the maximum diameter of three cisterns (insular cistern, longitudinal cerebral fissure and cerebral sulci greatest) with the temporal bones' greatest internal distance. This index, strongly related to age in healthy controls, is positively correlated to the preoperative and post-operative maximum diameter of hematoma and the midline shift in CSDH patients. On the contrary, it negatively correlates to the Karnofsky Performance Status (KPS). The Area Under the Receiver Operating Characteristics (AUROC) showed that RCA index effectively differentiated cases from controls. Immunohistochemistry analysis showed that the newly formed CD-31 positive microvessels are higher in number than the CD34-positive microvessels in the CSDH inner membrane than in the outer membrane. Ultrastructural observations highlight the presence of a chronic inflammatory state mainly in the CSDH inner membrane. Integrating these results, we have obtained an etiopathogenetic model of CSDH. Cortical atrophy appears to be the triggering factor activating the cascade of transendothelial cellular filtration, inflammation, membrane formation and neovascularisation leading to the CSDH formation.
几种理论试图阐明慢性硬脑膜下血肿(CSDH)病理生理学背后的机制。然而,这个过程很复杂,大部分仍然未知。在这项研究中,我们进行了一项回顾性随机分析,比较了 190 例单侧 CSDH 患者和 190 例健康对照组的皮质萎缩情况。为了评估皮质萎缩的程度,我们利用 CT 扫描图像开发了一个指数,即三个脑池最大直径总和与颞叶水平颅骨最大直径的比值。此外,我们首次报告了使用免疫组织化学方法和透射电子显微镜技术组合对 CSDH 的超微结构分析。进行了内部验证以确认对不同程度皮质萎缩的评估。相对皮质萎缩指数(RCA 指数)是指三个脑池(岛叶脑池、大脑纵裂和大脑沟最大)的最大直径与颞骨最大内距之和。这个指数与健康对照组的年龄密切相关,与 CSDH 患者术前和术后血肿的最大直径以及中线移位呈正相关。相反,它与卡诺夫斯基表现状态(KPS)呈负相关。接收器操作特征曲线下面积(AUROC)表明 RCA 指数可有效区分病例和对照组。免疫组织化学分析表明,新形成的 CD-31 阳性微血管数量比 CSDH 内膜中的 CD34 阳性微血管多。超微结构观察突出了慢性炎症状态的存在,主要存在于 CSDH 内膜中。综合这些结果,我们获得了 CSDH 的病因发病模型。皮质萎缩似乎是触发跨内皮细胞滤过、炎症、膜形成和新生血管形成级联反应导致 CSDH 形成的触发因素。