Department of Endocrinology, Skåne University Hospital, Lund University, 205 02 Malmö, Sweden.
Department of Immunology, Genetics, and Pathology; Uppsala University, 751 85 Uppsala, Sweden.
J Clin Endocrinol Metab. 2023 Jun 16;108(7):1585-1601. doi: 10.1210/clinem/dgad098.
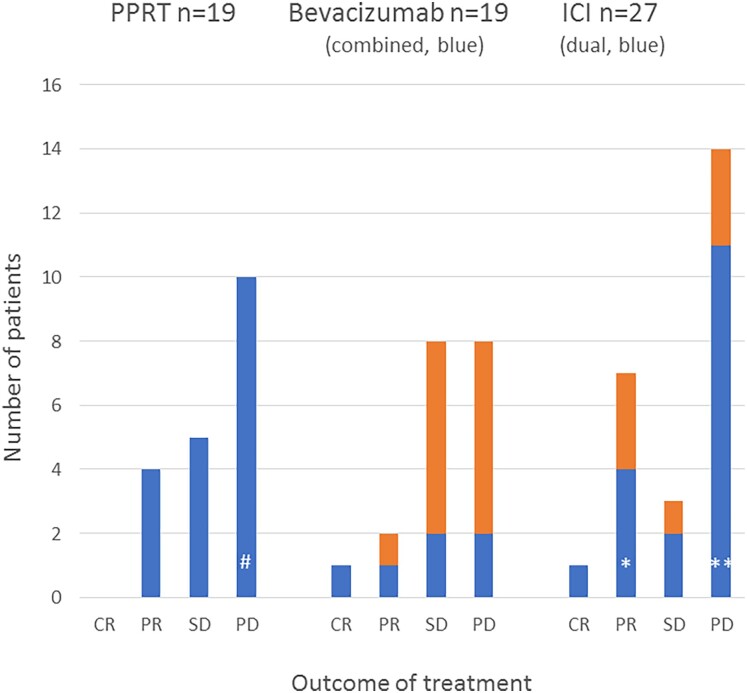
Aggressive pituitary tumors (APTs) and pituitary carcinomas (PCs) are heterogeneous with regard to clinical presentation, proliferative markers, clinical course, and response to therapy. Half of them show an aggressive course only many years after the first apparently benign presentation. APTs and PCs share several properties, but a Ki67 index greater than or equal to 10% and extensive p53 expression are more prevalent in PCs. Mutations in TP53 and ATRX are the most common genetic alterations; their detection might be of value for early identification of aggressiveness. Treatment requires a multimodal approach including surgery, radiotherapy, and drugs. Temozolomide is the recommended first-line chemotherapy, with response rates of about 40%. Immune checkpoint inhibitors have emerged as second-line treatment in PCs, with currently no evidence for a superior effect of dual therapy compared to monotherapy with PD-1 blockers. Bevacizumab has resulted in partial response (PR) in few patients; tyrosine kinase inhibitors and everolimus have generally not been useful. The effect of peptide receptor radionuclide therapy is limited as well. Management of APT/PC is challenging and should be discussed within an expert team with consideration of clinical and pathological findings, age, and general condition of the patient. Considering that APT/PCs are rare, new therapies should preferably be evaluated in shared standardized protocols. Prognostic and predictive markers to guide treatment decisions are needed and are the scope of ongoing research.
侵袭性垂体瘤(APTs)和垂体癌(PCs)在临床表现、增殖标志物、临床病程和对治疗的反应方面存在异质性。其中一半在首次表现为良性多年后才表现出侵袭性病程。APTs 和 PCs 具有一些共同特征,但 Ki67 指数大于或等于 10%和广泛的 p53 表达在 PCs 中更为常见。TP53 和 ATRX 基因突变是最常见的遗传改变;它们的检测可能对早期识别侵袭性具有重要意义。治疗需要多模式方法,包括手术、放疗和药物治疗。替莫唑胺是推荐的一线化疗药物,反应率约为 40%。免疫检查点抑制剂已成为 PCs 的二线治疗方法,目前尚无证据表明双药治疗比 PD-1 阻滞剂单药治疗效果更好。贝伐单抗在少数患者中产生部分缓解(PR);酪氨酸激酶抑制剂和依维莫司通常没有用。肽受体放射性核素治疗的效果也有限。APTs/PC 的治疗具有挑战性,应在专家团队中根据临床和病理发现、年龄和患者的一般状况进行讨论。鉴于 APT/PCs 较为罕见,新的治疗方法最好在共享的标准化方案中进行评估。需要有指导治疗决策的预后和预测标志物,这是正在进行的研究的范围。