Department of Neurosurgery, Beijing Tiantan Hospital, Capital Medical University, Beijing, China.
China National Clinical Research Center for Neurological Diseases, Beijing, China.
JAMA Netw Open. 2023 Mar 1;6(3):e231070. doi: 10.1001/jamanetworkopen.2023.1070.
The dilemma between natural rupture risk and adverse outcomes of intervention is of major concern for patients with unruptured arteriovenous malformations (AVMs). The existing risk score for AVM rupture includes factors that are controversial and lacks prospective validation.
To develop and robustly validate a reliable scoring system to predict the rupture risk of AVMs.
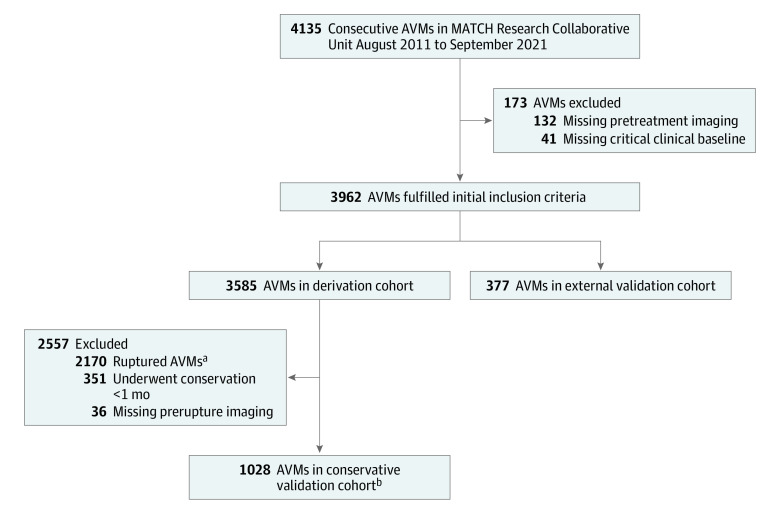
DESIGN, SETTING, AND PARTICIPANTS: This prognostic study developed a prediction model derived from a single-center cohort (derivation cohort) and validated in a multicenter external cohort (multicenter external validation cohort) and a cohort of patients receiving conservative treatment management (conservative treatment validation cohort). Patients were recruited from a nationwide multicenter prospective collaboration registry in China. A total of 4135 patients were enrolled in the registry between August 1, 2011, and September 1, 2021. Of those, 3962 patients were included in the study (3585 in the derivation cohort and 377 in the multicenter external validation cohort); 1028 patients from the derivation cohort who had time-to-event data and prerupture imaging results were included in the conservative treatment validation cohort. Data were analyzed from March 10 to June 21, 2022.
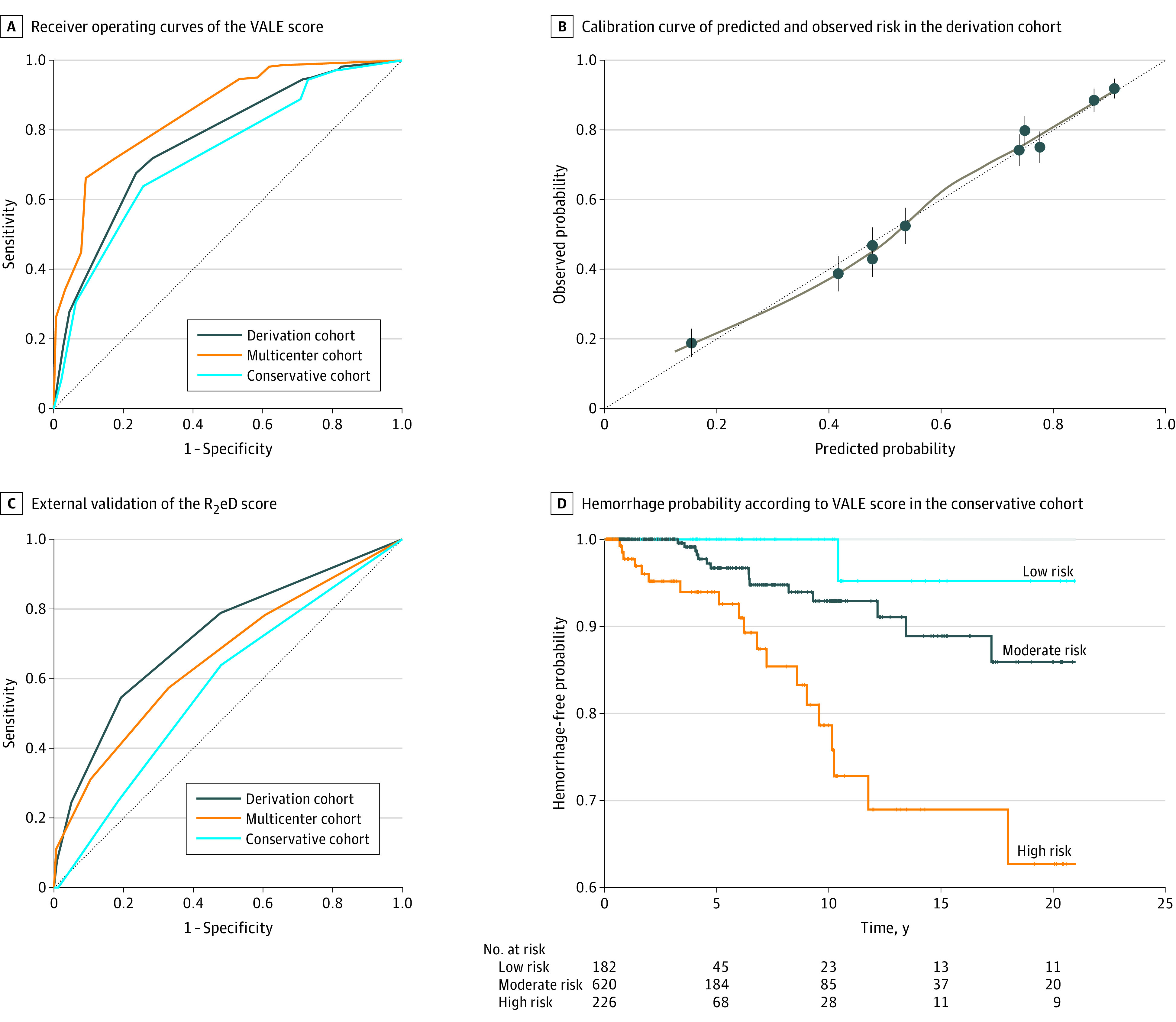
A scoring system was developed based on risk factors identified from a literature review and a robust selection process. Patients were stratified into different risk groups based on scores to calculate hemorrhage-free probability in future years, and Kaplan-Meier curves were plotted to visualize risk stratification. Receiver operating characteristic curves were used to assess the discrimination of models. Univariable analyses (logistic regression analysis for descriptive data and Cox regression analysis for survival data) were used to compare baseline information and assess bias.
Among 3962 patients (2311 men [58.3%]; median [IQR] age, 26.1 [14.6-35.5] years), 3585 patients (2100 men [58.6%]; median [IQR] age, 25.9 [14.6-35.0] years) were included in the derivation cohort, and 377 patients (211 men [56.0%]; median [IQR] age, 26.4 [14.5-39.2] years) were included in the multicenter external validation cohort. Thirty-six hemorrhages occurred over a median (IQR) follow-up of 4.2 (0.3-6.0) years among 1028 patients in the conservative treatment validation cohort. Four risk factors were used to develop the scoring system: ventricular system involvement, venous aneurysm, deep location, and exclusively deep drainage (VALE). The VALE scoring system performed well in all 3 cohorts, with areas under the receiver operating characteristic curve of 0.77 (95% CI, 0.75-0.78) in the derivation cohort, 0.85 (95% CI, 0.81-0.89) in the multicenter external validation cohort, and 0.73 (95% CI, 0.65-0.81) in the conservative treatment validation cohort. The 10-year hemorrhage-free rate was 95.5% (95% CI, 87.1%-100%) in the low-risk group, 92.8% (95% CI, 88.8%-97.0%) in the moderate-risk group, and 75.8% (95% CI, 65.1%-88.3%) in the high-risk group; the model discrimination was significant when comparing these rates between the high-risk group and the low- and moderate-risk groups (P < .001 for both comparisons).
In this prognostic study, the VALE scoring system was developed to distinguish rupture risk among patients with AVMs. The stratification of unruptured AVMs may enable patients with low risk of rupture to avoid unnecessary interventions. These findings suggest that the scoring system is a reliable and applicable tool that can be used to facilitate patient and physician decision-making and reduce unnecessary interventions or unexpected AVM ruptures.
动静脉畸形(AVM)未破裂患者所面临的自然破裂风险与干预不良后果之间的两难困境是主要关注点。现有的 AVM 破裂风险评分包括一些存在争议的因素,且缺乏前瞻性验证。
开发并稳健验证一种可靠的评分系统,以预测 AVM 破裂风险。
设计、设置和参与者:这项预后研究从单中心队列(推导队列)中开发了一种预测模型,并在多中心外部队列(多中心外部验证队列)和接受保守治疗管理的患者队列(保守治疗验证队列)中进行了验证。患者从中国全国多中心前瞻性协作登记处招募。2011 年 8 月 1 日至 2021 年 9 月 1 日期间,共有 4135 名患者入组该登记处。其中,3962 名患者纳入研究(3585 名在推导队列中,377 名在多中心外部验证队列中);3585 名推导队列中的 1028 名患者具有时间事件数据和破裂前影像学结果,被纳入保守治疗验证队列。数据分析于 2022 年 3 月 10 日至 6 月 21 日进行。
基于文献回顾和稳健选择过程中确定的风险因素,开发了一种评分系统。根据分数将患者分为不同的风险组,以计算未来几年的无出血概率,并绘制 Kaplan-Meier 曲线以可视化风险分层。使用受试者工作特征曲线评估模型的区分能力。单变量分析(用于描述性数据的逻辑回归分析和用于生存数据的 Cox 回归分析)用于比较基线信息并评估偏倚。
在 3962 名患者中(2311 名男性[58.3%];中位[IQR]年龄,26.1[14.6-35.5]岁),3585 名患者(2100 名男性[58.6%];中位[IQR]年龄,25.9[14.6-35.0]岁)被纳入推导队列,377 名患者(211 名男性[56.0%];中位[IQR]年龄,26.4[14.5-39.2]岁)被纳入多中心外部验证队列。在保守治疗验证队列的 1028 名患者中,中位(IQR)随访 4.2(0.3-6.0)年期间发生了 36 例出血。该评分系统使用 4 个风险因素进行开发:脑室系统受累、静脉瘤、深部位置和仅深部引流(VALE)。VALE 评分系统在所有 3 个队列中表现良好,推导队列中的受试者工作特征曲线下面积为 0.77(95%CI,0.75-0.78),多中心外部验证队列中的面积为 0.85(95%CI,0.81-0.89),保守治疗验证队列中的面积为 0.73(95%CI,0.65-0.81)。低风险组的 10 年无出血率为 95.5%(95%CI,87.1%-100%),中风险组为 92.8%(95%CI,88.8%-97.0%),高风险组为 75.8%(95%CI,65.1%-88.3%);当比较高风险组与低风险和中风险组之间的这些比率时,模型的区分度具有显著意义(两者之间的比较均 P<.001)。
在这项预后研究中,开发了 VALE 评分系统以区分 AVM 患者的破裂风险。未破裂 AVM 的分层可能使破裂风险低的患者能够避免不必要的干预。这些发现表明,该评分系统是一种可靠且适用的工具,可用于帮助患者和医生做出决策,并减少不必要的干预或意外的 AVM 破裂。