Department of Medical Oncology, Dana-Farber Cancer Institute, Boston, Massachusetts.
Oral Medicine Clinic, University of California San Francisco School of Dentistry, San Francisco, California.
Cancer Res Commun. 2021 Oct 13;1(1):30-40. doi: 10.1158/2767-9764.CRC-21-0060. eCollection 2021 Oct.
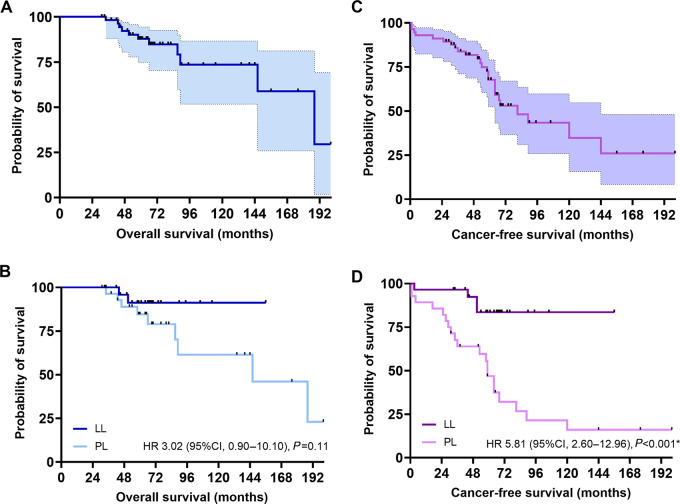
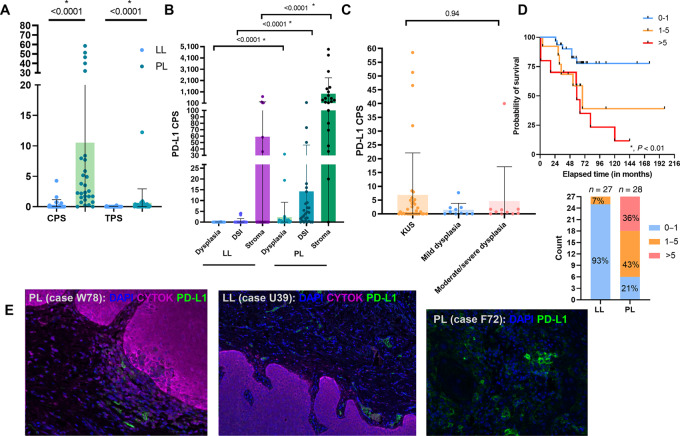
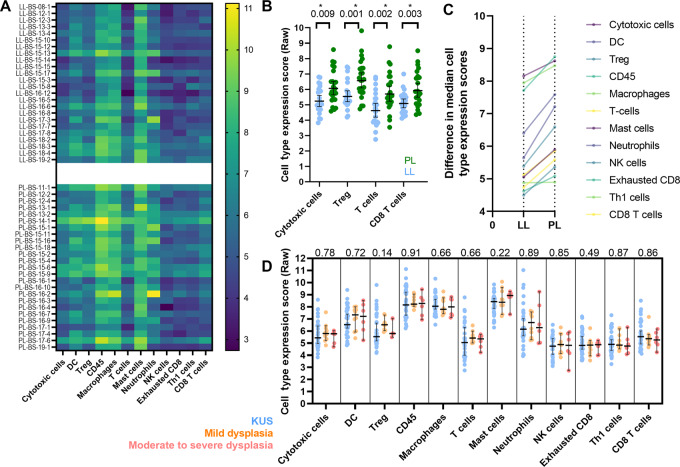
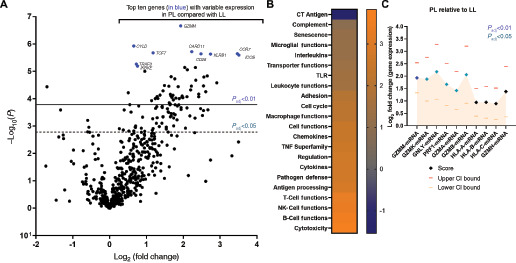
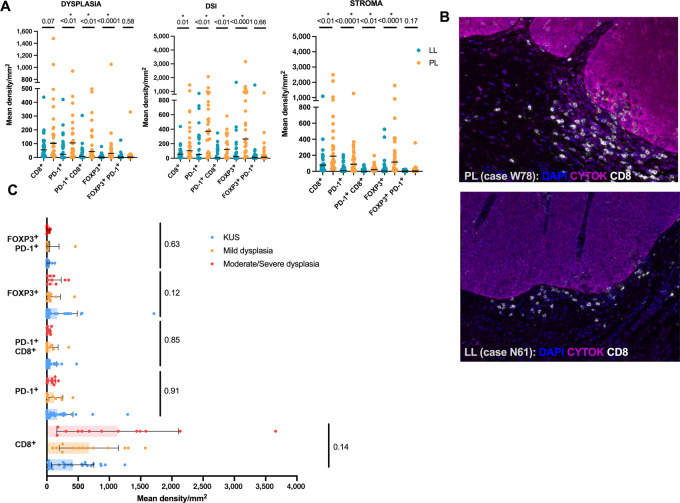
Oral leukoplakia is common and may, in some cases, progress to carcinoma. Proliferative leukoplakia is a progressive, often multifocal subtype with a high rate of malignant transformation compared with the more common localized leukoplakia. We hypothesized that the immune microenvironment and gene expression patterns would be distinct for proliferative leukoplakia compared with localized leukoplakia. We summarize key clinicopathologic features among proliferative leukoplakia and localized leukoplakia and compare cancer-free survival (CFS) between subgroups. We analyze immunologic gene expression profiling in proliferative leukoplakia and localized leukoplakia tissue samples (NanoString PanCancer Immune Oncology Profiling). We integrate immune cell activation and spatial distribution patterns in tissue samples using multiplexed immunofluorescence and digital image capture to further define proliferative leukoplakia and localized leukoplakia. Among = 58 patients (proliferative leukoplakia, = 29; localized leukoplakia, = 29), only the clinical diagnosis of proliferative leukoplakia was associated with significantly decreased CFS (HR, 11.25; < 0.01; 5-year CFS 46.8% and 83.6% among patients with proliferative leukoplakia and localized leukoplakia, respectively). CD8 T cells and T regulatory (Treg) were more abundant among proliferative leukoplakia samples ( < 0.01) regardless of degree of epithelial dysplasia, and often colocalized to the dysplasia-stromal interface. Gene set analysis identified granzyme M as the most differentially expressed gene favoring the proliferative leukoplakia subgroup (log fold change, 1.93; < 0.001). Programmed death ligand 1 (PD-L1) was comparatively overexpressed among proliferative leukoplakia samples, with higher (>5) PD-L1 scores predicting worse CFS ( < 0.01). Proliferative leukoplakia predicts a high rate of malignant transformation within 5 years of diagnosis. A prominent CD8 T-cell and Treg signature along with relative PD-L1 overexpression compared with localized leukoplakia provides strong rationale for PD-1/PD-L1 axis blockade using preventative immunotherapy.
This is the first in-depth profiling effort to immunologically characterize high-risk proliferative leukoplakia as compared with the more common localized leukoplakia. We observed a notable cytotoxic T-cell and Treg signature with relative overexpression of PD-L1 in high-risk proliferative leukoplakia providing a strong preclinical rationale for investigating PD-1/PD-L1 axis blockade in this disease as preventative immunotherapy.
口腔白斑病很常见,某些情况下可能会发展为癌。增殖性白斑病是一种进行性的、常为多灶性的亚型,与更常见的局限性白斑病相比,其恶性转化的发生率更高。我们假设增殖性白斑病与局限性白斑病的免疫微环境和基因表达模式会有所不同。我们总结了增殖性白斑病和局限性白斑病的关键临床病理特征,并比较了亚组间的无癌生存率(CFS)。我们分析了增殖性白斑病和局限性白斑病组织样本中的免疫基因表达谱(NanoString PanCancer Immune Oncology Profiling)。我们使用多重免疫荧光和数字图像捕获来整合组织样本中的免疫细胞激活和空间分布模式,以进一步定义增殖性白斑病和局限性白斑病。在 58 名患者中(增殖性白斑病患者 29 名,局限性白斑病患者 29 名),只有增殖性白斑病的临床诊断与显著降低的 CFS 相关(HR,11.25;<0.01;增殖性白斑病和局限性白斑病患者的 5 年 CFS 分别为 46.8%和 83.6%)。无论上皮异型程度如何,增殖性白斑病样本中 CD8 T 细胞和调节性 T 细胞(Treg)更为丰富(<0.01),并且常常与异型-基质界面共定位。基因集分析确定颗粒酶 M 是支持增殖性白斑病亚组的差异表达基因(log 倍数变化,1.93;<0.001)。与局限性白斑病相比,增殖性白斑病中程序性死亡配体 1(PD-L1)的表达相对较高,较高(>5)的 PD-L1 评分预示着更差的 CFS(<0.01)。增殖性白斑病在诊断后 5 年内有很高的恶性转化率。与更常见的局限性白斑病相比,增殖性白斑病中存在明显的 CD8 T 细胞和 Treg 特征,以及相对 PD-L1 的过度表达,这为使用预防性免疫疗法阻断 PD-1/PD-L1 轴提供了强有力的理由。
这是首次对高危增殖性白斑病进行深入的免疫特征分析,与更常见的局限性白斑病进行比较。我们观察到在高危增殖性白斑病中存在明显的细胞毒性 T 细胞和 Treg 特征,以及相对 PD-L1 的过度表达,这为在这种疾病中作为预防性免疫疗法研究 PD-1/PD-L1 轴阻断提供了强有力的临床前依据。