Department of Thoracic Medical Oncology, Shanghai Pulmonary Hospital, Tongji University School of Medicine, Shanghai, 200433, P. R. China.
Department of Respiratory Medicine, Harbin Medical University Cancer Hospital, Harbin, Heilongjiang, 150000, P. R. China.
Cancer Commun (Lond). 2022 Dec;42(12):1331-1346. doi: 10.1002/cac2.12383. Epub 2022 Nov 4.
Although programmed cell death 1 (PD-1) blockade plus chemotherapy can significantly prolong the progression-free survival (PFS) and overall survival (OS) in first-line settings in patients with driver-negative advanced non-small-cell lung cancer (NSCLC), the predictive biomarkers remain undetermined. Here, we investigated the predictive value of tumor immune microenvironmental marker expression to characterize the response features to PD-1 blockade plus chemotherapy.
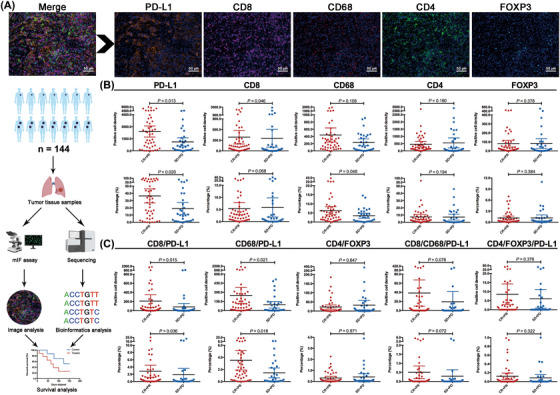
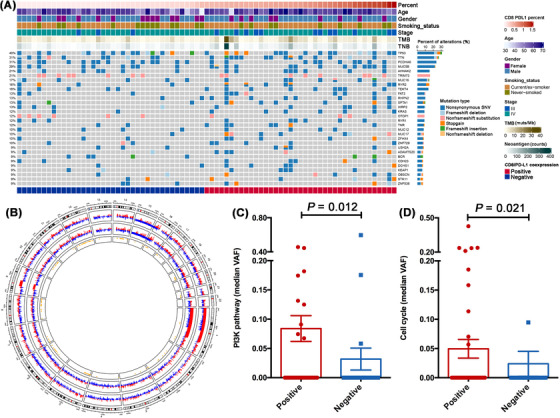
Tumor tissue samples at baseline were prospectively collected from 144 locally advanced or metastatic NSCLC patients without driver gene alterations who received camrelizumab plus chemotherapy or chemotherapy alone. Tumor immune microenvironmental markers, including PD-1 ligand (PD-L1), CD8, CD68, CD4 and forkhead box P3, were assessed using multiplex immunofluorescence (mIF) assays. Kaplan-Meier curves were used to determine treatment outcome differences according to their expression status. Mutational profiles were compared between tumors with distinct expression levels of these markers and their combinations.
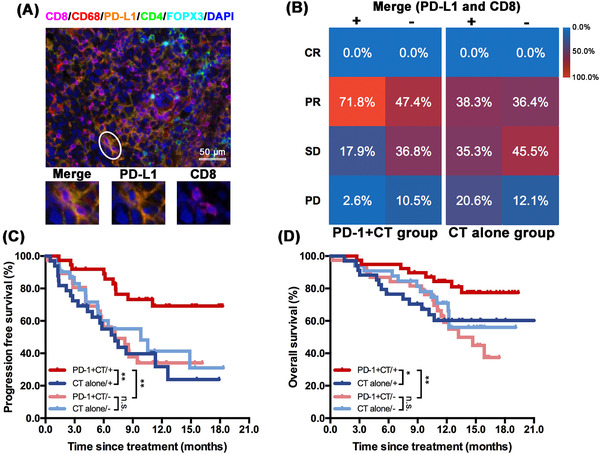
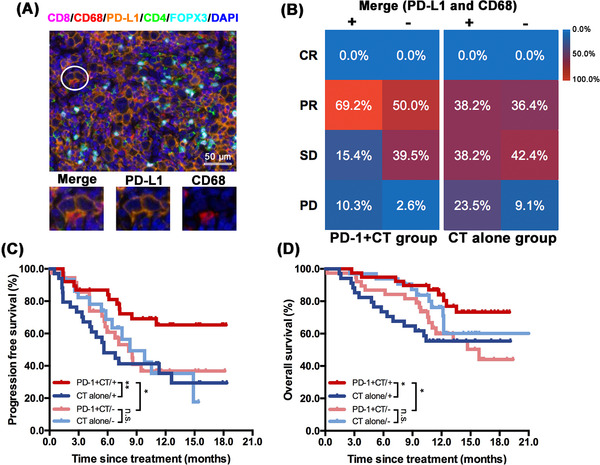
Responders had significantly higher CD8/PD-L1 (P = 0.015) or CD68/PD-L1 co-expression levels (P = 0.021) than non-responders in the camrelizumab plus chemotherapy group, while no difference was observed in the chemotherapy group. Patients with high CD8/PD-L1 or CD68/PD-L1 co-expression level was associated with significantly longer PFS (P = 0.002, P = 0.024; respectively) and OS (P = 0.006, P = 0.026; respectively) than those with low co-expression in camrelizumab plus chemotherapy group. When comparing survival in the camrelizumab plus chemotherapy with chemotherapy by CD8/PD-L1 co-expression stratification, significantly better PFS (P = 0.003) and OS (P = 0.032) were observed in high co-expression subgroups. The predictive value of CD8/PD-L1 and CD68/PD-L1 co-expression remained statistically significant for PFS and OS when adjusting clinicopathological features. Although the prevalence of TP53 or KRAS mutations was similar between patients with and without CD8/PD-L1 or CD68/PD-L1 co-expression, the positive groups had a significantly higher proportion of TP53/KRAS co-mutations than the negative groups (both 13.0% vs. 0.0%, P = 0.023). Notably, enriched PI3K (P = 0.012) and cell cycle pathway (P = 0.021) were found in the CD8/PD-L1 co-expression group.
Tumor immune microenvironmental marker expression, especially CD8/PD-L1 or CD68/PD-L1 co-expression, was associated with the efficacy of PD-1 blockade plus chemotherapy as first-line treatment in patients with advanced NSCLC.
程序性细胞死亡 1(PD-1)阻断联合化疗可显著延长驱动基因阴性晚期非小细胞肺癌(NSCLC)患者一线治疗中的无进展生存期(PFS)和总生存期(OS),但预测生物标志物仍未确定。在此,我们研究了肿瘤免疫微环境标志物表达的预测价值,以描述对 PD-1 阻断联合化疗的反应特征。
前瞻性收集 144 例无驱动基因突变的局部晚期或转移性 NSCLC 患者的基线肿瘤组织样本,这些患者接受卡瑞利珠单抗联合化疗或单纯化疗。使用多重免疫荧光(mIF)检测试剂盒评估肿瘤免疫微环境标志物,包括 PD-1 配体(PD-L1)、CD8、CD68、CD4 和叉头框 P3。根据表达状态,使用 Kaplan-Meier 曲线确定治疗结果差异。比较不同标志物及其组合表达水平的肿瘤之间的突变谱。
卡瑞利珠单抗联合化疗组中,应答者的 CD8/PD-L1(P=0.015)或 CD68/PD-L1 共表达水平显著高于无应答者,而化疗组无差异。高 CD8/PD-L1 或 CD68/PD-L1 共表达水平与卡瑞利珠单抗联合化疗组患者的 PFS(P=0.002,P=0.024)和 OS(P=0.006,P=0.026)显著延长相关,而低共表达水平与较短的 PFS(P=0.002,P=0.024)和 OS(P=0.006,P=0.026)相关。当按 CD8/PD-L1 共表达分层比较卡瑞利珠单抗联合化疗与化疗的生存情况时,在高共表达亚组中,PFS(P=0.003)和 OS(P=0.032)的改善具有统计学意义。调整临床病理特征后,CD8/PD-L1 和 CD68/PD-L1 共表达对 PFS 和 OS 的预测价值仍然具有统计学意义。尽管 CD8/PD-L1 或 CD68/PD-L1 共表达患者与无共表达患者之间的 TP53 或 KRAS 突变发生率相似,但阳性组的 TP53/KRAS 共突变比例明显高于阴性组(均为 13.0% vs. 0.0%,P=0.023)。值得注意的是,在 CD8/PD-L1 共表达组中发现了丰富的 PI3K(P=0.012)和细胞周期途径(P=0.021)。
肿瘤免疫微环境标志物表达,尤其是 CD8/PD-L1 或 CD68/PD-L1 共表达,与 PD-1 阻断联合化疗作为晚期 NSCLC 一线治疗的疗效相关。