University of Chicago Pritzker School of Medicine, Chicago, IL, USA.
University of Chicago Section of General Internal Medicine, Chicago, IL, USA.
J Gen Intern Med. 2023 Mar;38(Suppl 1):48-55. doi: 10.1007/s11606-022-07918-2. Epub 2023 Mar 2.
Global budgets might incentivize healthcare systems to develop population health programs to prevent costly hospitalizations. In response to Maryland's all-payer global budget financing system, University of Pittsburgh Medical Center (UPMC) Western Maryland developed an outpatient care management center called the Center for Clinical Resources (CCR) to support high-risk patients with chronic disease.
Evaluate the impact of the CCR on patient-reported, clinical, and resource utilization outcomes for high-risk rural patients with diabetes.
Observational cohort study.
One hundred forty-one adult patients with uncontrolled diabetes (HbA1c > 7%) and one or more social needs who were enrolled between 2018 and 2021.
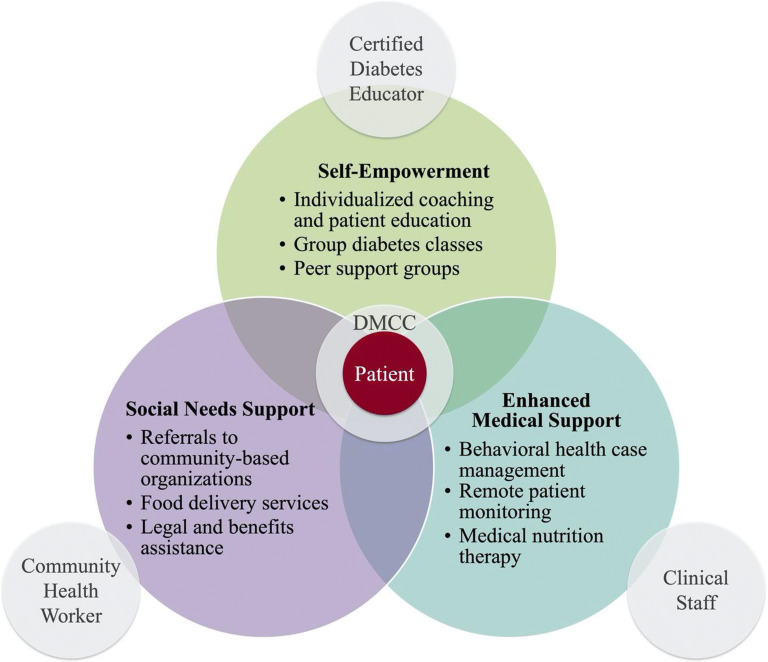
Team-based interventions that provided interdisciplinary care coordination (e.g., diabetes care coordinators), social needs support (e.g., food delivery, benefits assistance), and patient education (e.g., nutritional counseling, peer support).
Patient-reported (e.g., quality of life, self-efficacy), clinical (e.g., HbA1c), and utilization outcomes (e.g., emergency department visits, hospitalizations).
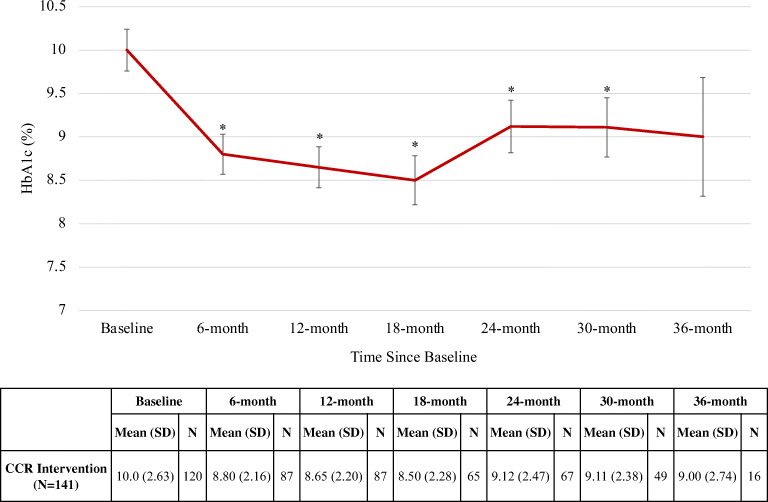
Patient-reported outcomes improved significantly at 12 months, including confidence in self-management, quality of life, and patient experience (56% response rate). No significant demographic differences were detected between patients with or without the 12-month survey response. Baseline mean HbA1c was 10.0% and decreased on average by 1.2 percentage points at 6 months, 1.4 points at 12 months, 1.5 points at 18 months, and 0.9 points at 24 and 30 months (P<0.001 at all timepoints). No significant changes were observed in blood pressure, low-density lipoprotein cholesterol, or weight. The annual all-cause hospitalization rate decreased by 11 percentage points (34 to 23%, P=0.01) and diabetes-related emergency department visits also decreased by 11 percentage points (14 to 3%, P=0.002) at 12 months.
CCR participation was associated with improved patient-reported outcomes, glycemic control, and hospital utilization for high-risk patients with diabetes. Payment arrangements like global budgets can support the development and sustainability of innovative diabetes care models.
全球预算可能会激励医疗系统制定人口健康计划,以预防昂贵的住院治疗。为了应对马里兰州的全民支付全球预算融资系统,匹兹堡大学医学中心(UPMC)西部马里兰州成立了一个名为临床资源中心(CCR)的门诊护理管理中心,为患有慢性病的高危患者提供支持。
评估 CCR 对患有糖尿病的高危农村患者的患者报告、临床和资源利用结果的影响。
观察性队列研究。
2018 年至 2021 年间入组的 141 名未控制的糖尿病(HbA1c > 7%)且有一个或多个社会需求的成年患者。
提供跨学科护理协调(例如,糖尿病护理协调员)、社会需求支持(例如,食品配送、福利援助)和患者教育(例如,营养咨询、同伴支持)的团队干预措施。
患者报告的结果(例如,生活质量、自我效能感)、临床结果(例如,HbA1c)和利用结果(例如,急诊就诊、住院治疗)。
12 个月时患者报告的结果显著改善,包括自我管理信心、生活质量和患者体验(56%的回复率)。在是否有 12 个月调查回复方面,患者之间没有发现显著的人口统计学差异。基线平均 HbA1c 为 10.0%,6 个月时平均降低 1.2 个百分点,12 个月时降低 1.4 个百分点,18 个月时降低 1.5 个百分点,24 个月和 30 个月时降低 0.9 个百分点(所有时间点均 P<0.001)。血压、低密度脂蛋白胆固醇或体重无显著变化。全因住院率下降了 11 个百分点(34%降至 23%,P=0.01),糖尿病相关急诊就诊率也下降了 11 个百分点(14%降至 3%,P=0.002),均发生在 12 个月时。
CCR 的参与与高危糖尿病患者的患者报告结果、血糖控制和住院利用率的改善有关。像全球预算这样的支付安排可以支持创新的糖尿病护理模式的发展和可持续性。