Zhou Wanshu, Sabel Bernhard A
Institute of Medical Psychology, Medical Faculty, Otto-Von-Guericke University of Magdeburg, Leipziger Straße 44, 39120 Magdeburg, Germany.
EPMA J. 2023 Feb 16;14(1):87-99. doi: 10.1007/s13167-023-00316-6. eCollection 2023 Mar.
Vision loss in glaucoma is not only associated with elevated intraocular pressure and neurodegeneration, but vascular dysregulation (VD) is a major factor. To optimize therapy, an improved understanding of concepts of predictive, preventive, and personalized medicine (3PM) is needed which is based on a more detailed understanding of VD pathology. Specifically, to learn if the root cause of glaucomatous vision loss is of neuronal (degeneration) or vascular origin, we now studied neurovascular coupling (NVC) and vessel morphology and their relationship to vision loss in glaucoma.
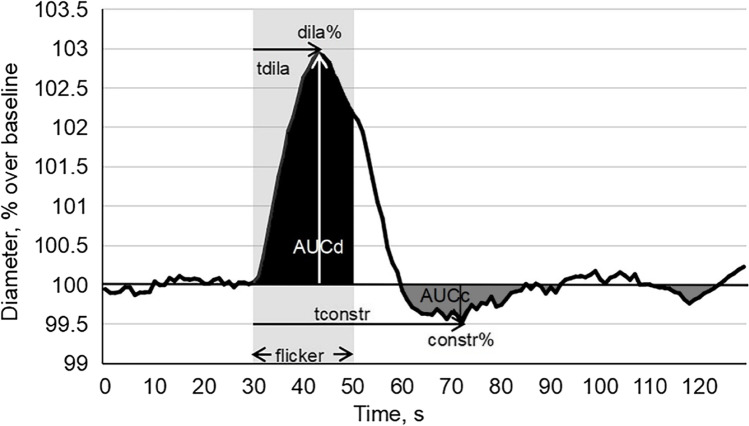
In patients with primary open angle glaucoma (POAG) ( = 30) and healthy controls ( = 22), NVC was studied using dynamic vessel analyzer to quantify retinal vessel diameter before, during, and after flicker light stimulation to evaluate the dilation response following neuronal activation. Vessel features and dilation were then related to branch level and visual field impairment.
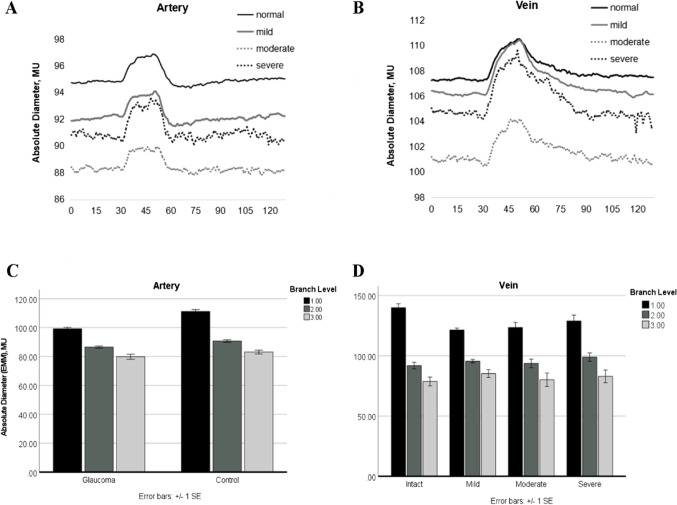
Retinal arterial and venous vessels had significantly smaller diameters in patients with POAG in comparison to controls. However, both arterial and venous dilation reached normal values during neuronal activation despite their smaller diameters. This was largely independent of visual field depth and varied among patients.
Because dilation/constriction is normal, VD in POAG can be explained by chronic vasoconstriction which limits energy supply to retinal (and brain) neurons with subsequent hypo-metabolism ("silent" neurons) or neuronal cell death. We propose that the root cause of POAG is primarily of vascular and not neuronal origin. This understanding can help to better personalize POAG therapy of not only targeting eye pressure but also vasoconstriction to prevent low vision, slowing its progression and supporting recovery and restoration.
ClinicalTrials.gov, # NCT04037384 on July 3, 2019.
青光眼导致的视力丧失不仅与眼压升高和神经退行性变有关,而且血管调节功能障碍(VD)也是一个主要因素。为了优化治疗,需要在更详细了解VD病理的基础上,更好地理解预测、预防和个性化医学(3PM)的概念。具体而言,为了弄清楚青光眼性视力丧失的根本原因是神经元(变性)还是血管源性,我们现在研究了神经血管耦合(NVC)和血管形态及其与青光眼视力丧失的关系。
在原发性开角型青光眼(POAG)患者(n = 30)和健康对照者(n = 22)中,使用动态血管分析仪研究NVC,以量化闪烁光刺激前、期间和之后的视网膜血管直径,评估神经元激活后的扩张反应。然后将血管特征和扩张与分支水平和视野损害相关联。
与对照组相比,POAG患者的视网膜动脉和静脉血管直径明显较小。然而,尽管它们的直径较小,但在神经元激活期间,动脉和静脉扩张均达到正常值。这在很大程度上与视野深度无关,且患者之间存在差异。
由于扩张/收缩正常,POAG中的VD可以用慢性血管收缩来解释,慢性血管收缩限制了视网膜(和大脑)神经元的能量供应,随后出现代谢减退(“沉默”神经元)或神经元细胞死亡。我们提出,POAG的根本原因主要是血管源性而非神经元源性。这种认识有助于更好地对POAG治疗进行个性化,不仅针对眼压,还针对血管收缩,以预防低视力,减缓其进展并支持恢复和康复。
ClinicalTrials.gov,# NCT04037384,2019年7月3日。