Research Centre for Hauora and Health, Massey University, Wellington, New Zealand.
Department of Medicine, University of Otago Wellington, Wellington, New Zealand.
Int J Stroke. 2023 Jul;18(6):663-671. doi: 10.1177/17474930231164024. Epub 2023 Mar 24.
Ethnic differences in post-stroke outcomes have been largely attributed to biological and socioeconomic characteristics resulting in differential risk factor profiles and stroke subtypes, but evidence is mixed.
This study assessed ethnic differences in stroke outcome and service access in New Zealand (NZ) and explored underlying causes in addition to traditional risk factors.
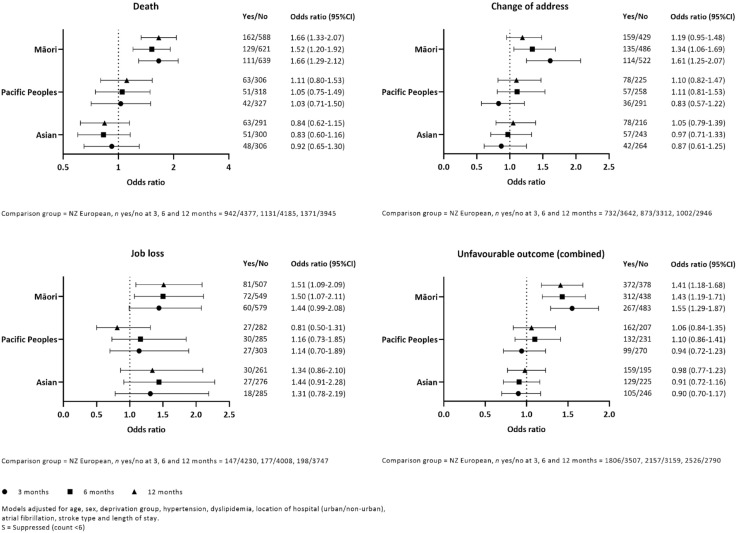
This national cohort study used routinely collected health and social data to compare post-stroke outcomes between NZ Europeans, Māori, Pacific Peoples, and Asians, adjusting for differences in baseline characteristics, socioeconomic deprivation, and stroke characteristics. First and principal stroke public hospital admissions during November 2017 to October 2018 were included (N = 6879). Post-stroke unfavorable outcome was defined as being dead, changing residence, or becoming unemployed.
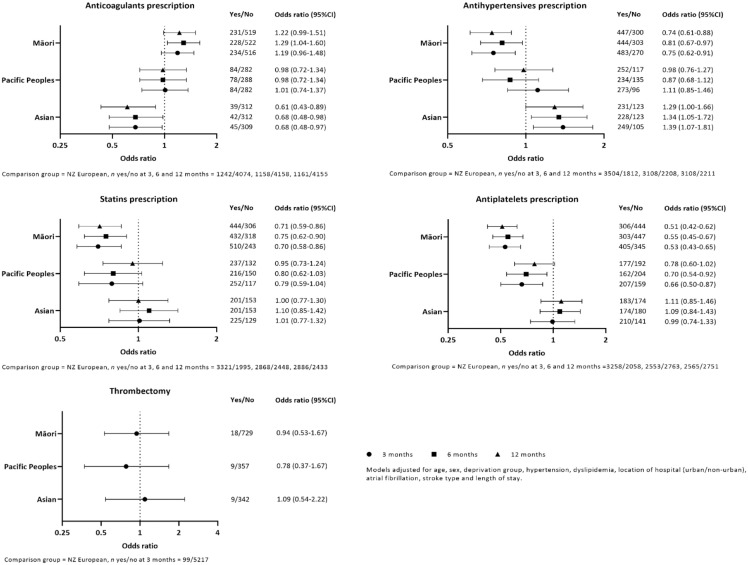
In total, 5394 NZ Europeans, 762 Māori, 369 Pacific Peoples, and 354 Asians experienced a stroke during the study period. Median age was 65 years for Māori and Pacific Peoples, and 71 and 79 years for Asians and NZ Europeans, respectively. Compared with NZ Europeans, Māori were more likely to have an unfavorable outcome at all three time-points (odds ratio (OR) = 1.6 (95% confidence interval (CI) = 1.3-1.9); 1.4 (1.2-1.7); 1.4 (1.2-1.7), respectively). Māori had increased odds of death at all time-points (1.7 (1.3-2.1); 1.5 (1.2-1.9); 1.7 (1.3-2.1)), change in residence at 3 and 6 months (1.6 (1.3-2.1); 1.3 (1.1-1.7)), and unemployment at 6 and 12 months (1.5 (1.1-2.1); 1.5 (1.1-2.1)). There was evidence of differences in post-stroke secondary prevention medication by ethnicity.
We found ethnic disparities in care and outcomes following stroke which were independent of traditional risk factors, suggesting they may be attributable to stroke service delivery rather than patient factors.
脑卒中后结局的种族差异主要归因于生物学和社会经济特征,导致不同的危险因素谱和脑卒中亚型,但证据不一。
本研究评估了新西兰(NZ)脑卒中结局和服务获取方面的种族差异,并探讨了除传统危险因素以外的潜在原因。
本项全国性队列研究使用常规收集的健康和社会数据,比较了 2017 年 11 月至 2018 年 10 月期间 NZ 欧洲人、毛利人、太平洋岛民和亚洲人之间的脑卒中后结局,调整了基线特征、社会经济剥夺和脑卒中特征的差异。纳入首次和主要因脑卒中住院的患者(N=6879)。脑卒中后不良结局定义为死亡、改变居住地或失业。
研究期间,共有 5394 名 NZ 欧洲人、762 名毛利人、369 名太平洋岛民和 354 名亚洲人发生脑卒中。毛利人和太平洋岛民的中位年龄为 65 岁,亚洲人和 NZ 欧洲人的中位年龄分别为 71 岁和 79 岁。与 NZ 欧洲人相比,毛利人在所有三个时间点都更有可能出现不良结局(优势比(OR)=1.6(95%置信区间(CI)=1.3-1.9);1.4(1.2-1.7);1.4(1.2-1.7))。毛利人在所有时间点的死亡风险都更高(1.7(1.3-2.1);1.5(1.2-1.9);1.7(1.3-2.1)),3 个月和 6 个月时居住地改变的风险(1.6(1.3-2.1);1.3(1.1-1.7)),6 个月和 12 个月时失业风险(1.5(1.1-2.1);1.5(1.1-2.1))。不同种族在脑卒中二级预防药物治疗方面存在差异。
我们发现脑卒中后护理和结局存在种族差异,这与传统危险因素无关,表明这可能归因于脑卒中服务提供而非患者因素。