de Barros Hilda A, Duin Jan J, Mulder Daan, van der Noort Vincent, Noordzij M Arjen, Wit Esther M K, Pos Floris J, Vogel Wouter V, Schaake Eva E, van Leeuwen Fijs W B, van Leeuwen Pim J, Grivas Nikolaos, van der Poel Henk G
Department of Urology, The Netherlands Cancer Institute-Antoni van Leeuwenhoek Hospital, Amsterdam, The Netherlands.
Prostate Cancer Network the Netherlands, Amsterdam, The Netherlands.
Eur Urol Open Sci. 2023 Jan 30;49:80-89. doi: 10.1016/j.euros.2022.12.011. eCollection 2023 Mar.
Accurate identification of men who harbor nodal metastases is necessary to select patients who most likely benefit from whole pelvis radiotherapy (WPRT). Limited sensitivity of diagnostic imaging approaches for the detection of nodal micrometastases has led to the exploration of the sentinel lymph node biopsy (SLNB).
To evaluate whether SLNB can be used as a tool to select pathologically node-positive patients who likely benefit from WPRT.
We included 528 clinically node-negative primary prostate cancer (PCa) patients with an estimated nodal risk of >5% treated between 2007 and 2018.
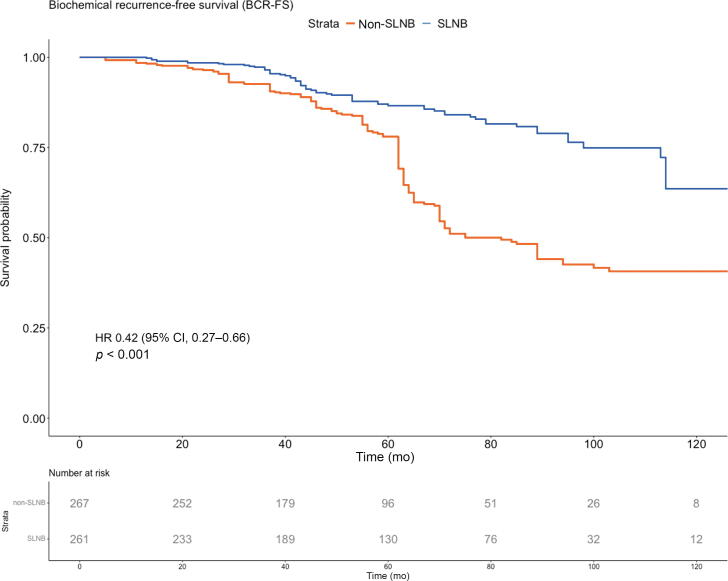
A total of 267 patients were directly treated with prostate-only radiotherapy (PORT; non-SLNB group), while 261 patients underwent SLNB to remove lymph nodes directly draining from the primary tumor prior to radiotherapy (SLNB group); pN0 patients were treated with PORT, while pN1 patients were offered WPRT.
Biochemical recurrence-free survival (BCRFS) and radiological recurrence-free survival (RRFS) were compared using propensity score weighted (PSW) Cox proportional hazard models.
The median follow-up was 71 mo. Occult nodal metastases were found in 97 (37%) SLNB patients (median metastasis size: 2 mm). Adjusted 7-yr BCRFS rates were 81% (95% confidence interval [CI] 77-86%) in the SLNB group and 49% (95% CI 43-56%) in the non-SLNB group. The corresponding adjusted 7-yr RRFS rates were 83% (95% CI 78-87%) and 52% (95% CI 46-59%), respectively. In the PSW multivariable Cox regression analysis, SLNB was associated with improved BCRFS (hazard ratio [HR] 0.38, 95% CI 0.25-0.59, < 0.001) and RRFS (HR 0.44, 95% CI 0.28-0.69, < 0.001). Limitations include the bias inherent to the study's retrospective nature.
SLNB-based selection of pN1 PCa patients for WPRT was associated with significantly improved BCRFS and RRFS compared with (conventional) imaging-based PORT.
Sentinel node biopsy can be used to select patients who will benefit from the addition of pelvis radiotherapy. This strategy results in a longer duration of prostate-specific antigen control and a lower risk of radiological recurrence.
准确识别有淋巴结转移的男性对于选择最有可能从全盆腔放疗(WPRT)中获益的患者至关重要。诊断性成像方法检测淋巴结微转移的敏感性有限,这促使人们探索前哨淋巴结活检(SLNB)。
评估SLNB是否可作为一种工具,用于选择可能从WPRT中获益的病理淋巴结阳性患者。
设计、设置和参与者:我们纳入了2007年至2018年间接受治疗的528例临床淋巴结阴性的原发性前列腺癌(PCa)患者,其估计淋巴结转移风险>5%。
总共267例患者直接接受仅前列腺放疗(PORT;非SLNB组),而261例患者在放疗前接受SLNB以切除直接引流原发性肿瘤的淋巴结(SLNB组);pN0患者接受PORT治疗,而pN1患者接受WPRT。
使用倾向评分加权(PSW)Cox比例风险模型比较生化无复发生存期(BCRFS)和放射学无复发生存期(RRFS)。
中位随访时间为71个月。在97例(37%)SLNB患者中发现隐匿性淋巴结转移(转移灶大小中位数:2mm)。SLNB组调整后的7年BCRFS率为81%(95%置信区间[CI]77 - 86%),非SLNB组为49%(95%CI 43 - 56%)。相应的调整后7年RRFS率分别为83%(95%CI 78 - 87%)和52%(95%CI 46 - 59%)。在PSW多变量Cox回归分析中,SLNB与改善的BCRFS(风险比[HR]0.38,95%CI 0.25 - 0.59,<0.001)和RRFS(HR 0.44,95%CI 0.28 - 0.69,<0.001)相关。局限性包括该研究回顾性性质所固有的偏倚。
与基于(传统)成像的PORT相比,基于SLNB选择pN1 PCa患者进行WPRT与显著改善的BCRFS和RRFS相关。
前哨淋巴结活检可用于选择将从盆腔放疗加用中获益的患者。这种策略导致前列腺特异性抗原控制时间更长,放射学复发风险更低。