Division of Oncology/Unit of Urology, URI, IRCCS Ospedale San Raffaele, Milan, Italy.
Department of Urology, Policlinico San Martino Hospital, University of Genova, Genova, Italy.
Eur Urol. 2020 Nov;78(5):661-669. doi: 10.1016/j.eururo.2020.06.043. Epub 2020 Jul 2.
Long-term outcomes of patients treated with salvage lymph node dissection (sLND) for nodal recurrence of prostate cancer (PCa) remain unknown.
To investigate long-term oncological outcomes after sLND in a large multi-institutional series.
DESIGN, SETTING, AND PARTICIPANTS: The study included 189 patients who experienced prostate-specific antigen (PSA) rise and nodal-only recurrence after radical prostatectomy (RP) and underwent sLND at 11 tertiary referral centers between 2002 and 2011. Lymph node recurrence was documented by positron emission tomography/computed tomography (PET/CT) scan using either C-choline or Ga prostate-specific membrane antigen ligand.
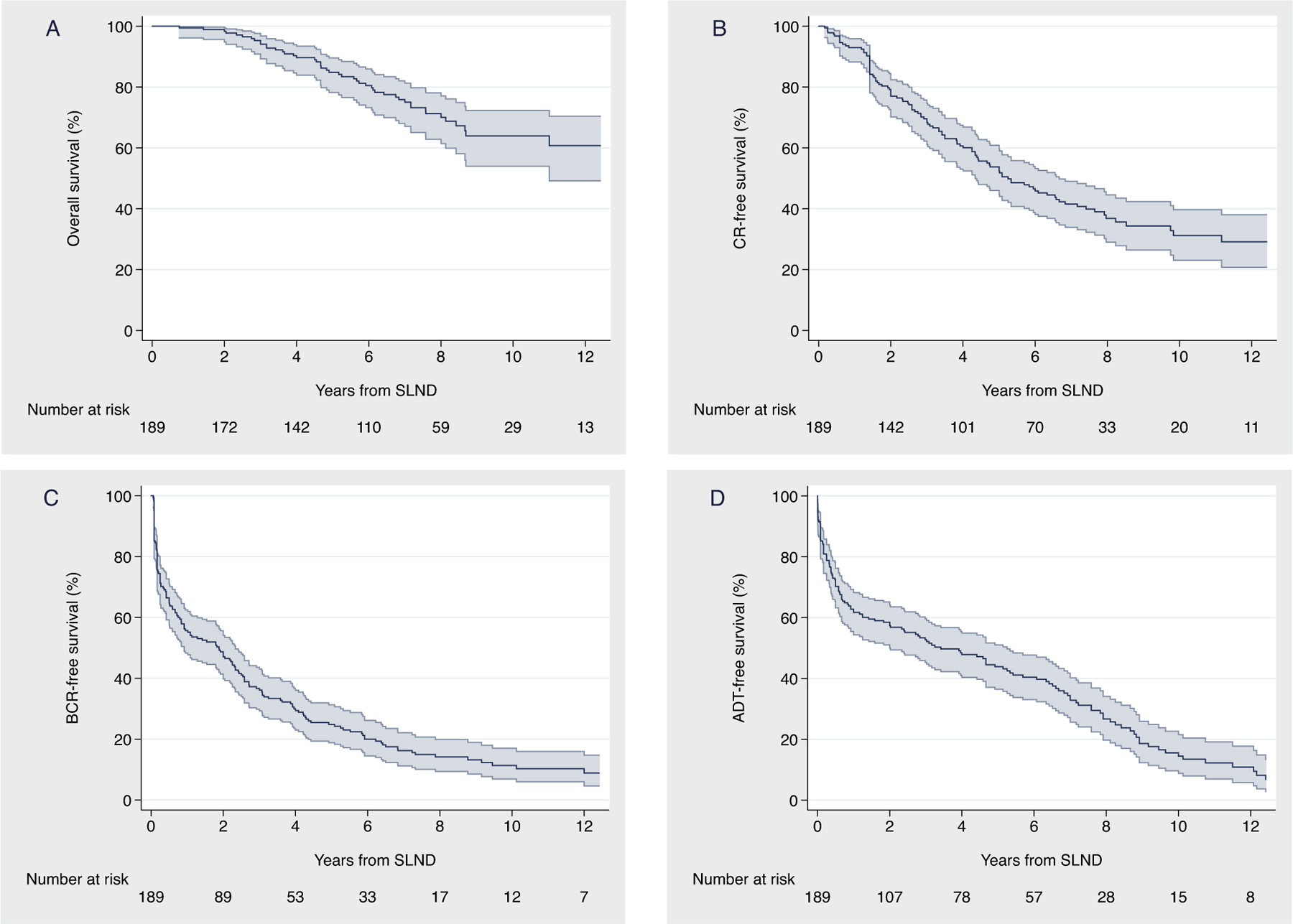
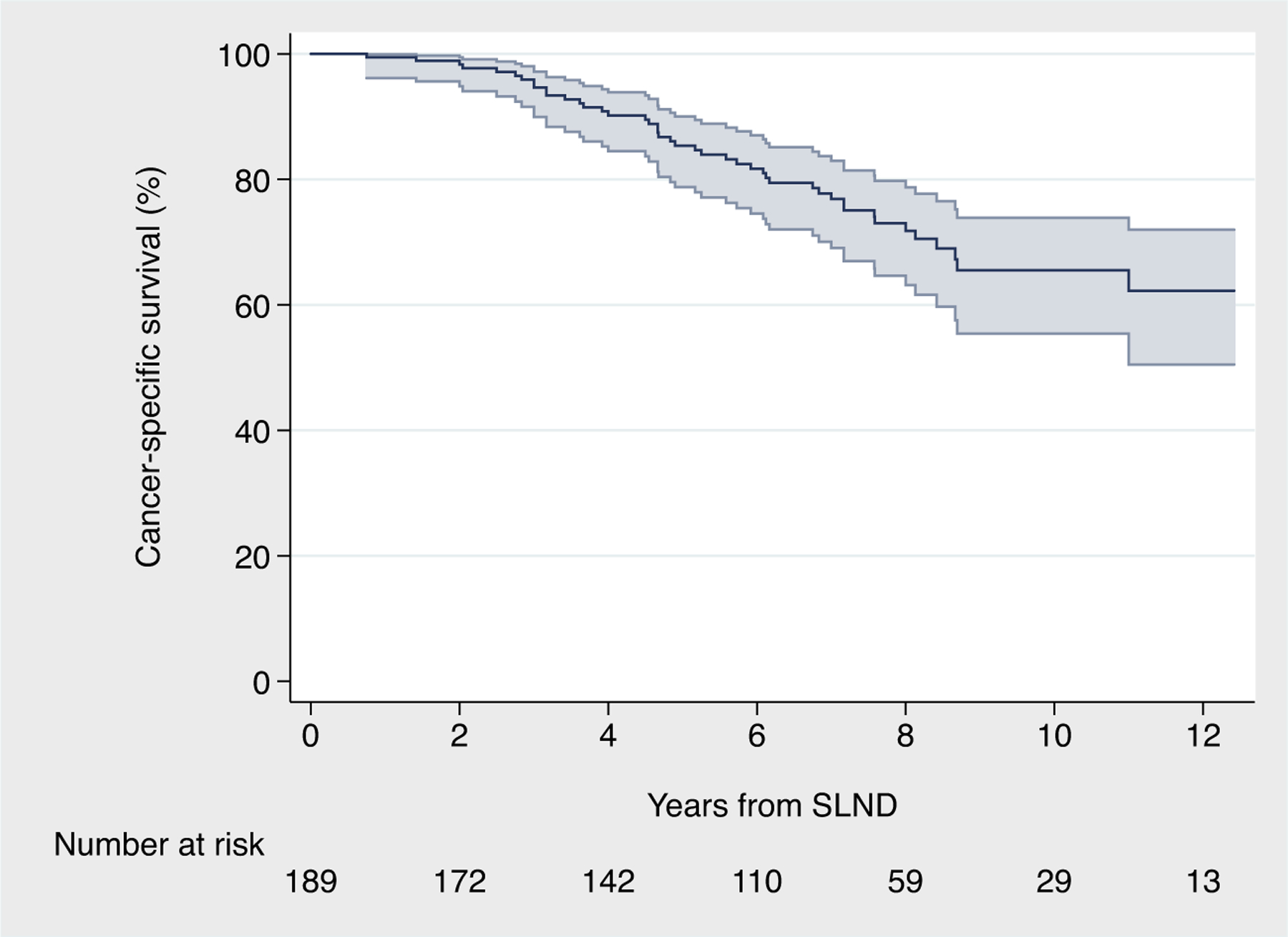
The primary outcome of the study was cancer-specific mortality (CSM). The secondary outcomes were overall mortality, clinical recurrence (CR), biochemical recurrence (BCR), and androgen deprivation therapy (ADT)-free survival after sLND. The probability of freedom from each outcome was calculated using Kaplan-Meier analyses. Cox regression analysis was used to predict the risk of prostate CSM after accounting for several parameters, including the use of additional treatments after sLND.
At long term, 110 and 163 patients experienced CR and BCR, respectively, with CR-free and BCR-free survival at 10 yr of 31% and 11%, respectively. After sLND, a total of 145 patients received ADT, with a median time to ADT of 41 mo. At a median (interquartile range) follow-up for survivors of 87 (51, 104) mo, 48 patients died. Of them, 45 died from PCa. The probabilities of freedom from cancer-specific and all-cause death at 10 yr were 66% and 64%, respectively. Similar results were obtained in sensitivity analyses in patients with pelvic-only positive PET/CT scan, as well as after excluding men on ADT at PET/CT scan and patients with PSA level at sLND higher than the 75th percentile. At multivariable analyses, patients who had PSA response after sLND (hazard ratio [HR]: 0.45; p = 0.001), and those receiving ADT within 6 mo from sLND (HR: 0.51; p = 0.010) had lower risk of death from PCa.
A third of men treated with sLND for PET-detected nodal recurrence of PCa died at long term, with PCa being the main cause of death. Salvage LND alone was associated with durable long-term outcomes in a minority of men who significantly benefited from additional treatments after surgery. Taken together, all these data argue against the use of metastasis-directed therapy alone for patients with node-only recurrent PCa. These men should instead be considered at high risk of systemic dissemination already at the time of sLND.
We assessed long-term outcomes of patients treated with salvage lymph node dissection (sLND) for node-recurrent prostate cancer (PCa). In contrast with prior evidence, we found that the majority of these men recurred after sLND and eventually died from PCa. A significant survival benefit associated with the administration of androgen deprivation therapy after sLND suggests that sLND should be considered part of a multimodal approach rather than an exclusive treatment strategy.
接受挽救性淋巴结清扫术(sLND)治疗前列腺癌(PCa)淋巴结复发患者的长期预后尚不清楚。
在一个大型多机构系列中,研究 sLND 后的长期肿瘤学结局。
设计、地点和参与者:这项研究纳入了 189 名患者,他们在根治性前列腺切除术(RP)后出现前列腺特异性抗原(PSA)升高和仅淋巴结复发,并在 2002 年至 2011 年期间在 11 个三级转诊中心接受 sLND。通过正电子发射断层扫描/计算机断层扫描(PET/CT)扫描使用 C-胆碱或 Ga 前列腺特异性膜抗原配体检测到淋巴结复发。
研究的主要结局是癌症特异性死亡率(CSM)。次要结局是总死亡率、临床复发(CR)、生化复发(BCR)和 sLND 后无雄激素剥夺治疗(ADT)生存。使用 Kaplan-Meier 分析计算每个结局的无事件概率。Cox 回归分析用于预测 sLND 后前列腺 CSM 的风险,同时考虑了包括 sLND 后使用额外治疗在内的几个参数。
长期随访时,110 名患者出现 CR,163 名患者出现 BCR,10 年时 CR 无复发和 BCR 无复发的生存率分别为 31%和 11%。sLND 后,共有 145 名患者接受 ADT,中位 ADT 时间为 41 个月。在幸存者的中位(四分位间距)随访 87(51,104)个月时,48 名患者死亡。其中,45 人死于 PCa。10 年时无癌症特异性和全因死亡的概率分别为 66%和 64%。在仅盆腔阳性 PET/CT 扫描患者的敏感性分析以及在排除 PET/CT 扫描时接受 ADT 的患者和 sLND 时 PSA 水平高于第 75 百分位数的患者的敏感性分析中,均获得了相似的结果。多变量分析显示,sLND 后 PSA 有反应的患者(风险比 [HR]:0.45;p=0.001)和 sLND 后 6 个月内接受 ADT 的患者(HR:0.51;p=0.010)的 PCa 死亡风险较低。
接受 sLND 治疗 PET 检测到的 PCa 淋巴结复发的患者中有三分之一在长期随访中死亡,PCa 是主要死因。单独的挽救性淋巴结清扫术与少数接受手术后额外治疗的患者的长期生存有关,这些患者从中显著获益。综合所有这些数据,反对单独使用针对转移的治疗方法治疗仅淋巴结复发的 PCa 患者。这些患者在接受 sLND 时已经处于全身扩散的高风险中。
我们评估了接受挽救性淋巴结清扫术(sLND)治疗淋巴结复发性前列腺癌(PCa)患者的长期预后。与之前的证据不同,我们发现大多数患者在 sLND 后复发,最终死于 PCa。sLND 后接受雄激素剥夺治疗与生存获益显著相关,提示 sLND 应被视为多模式治疗的一部分,而不是单独的治疗策略。