Department of Pulmonary and Critical Care Medicine, Center of Respiratory Medicine, National Center for Respiratory Medicine, China-Japan Friendship Hospital, Beijing, China.
Capital Medical University, China-Japan Friendship School of Clinical Medicine, Beijing, China.
Front Public Health. 2023 Feb 15;11:1070581. doi: 10.3389/fpubh.2023.1070581. eCollection 2023.
Immunocompromised patients with severe community-acquired pneumonia (SCAP) warrant special attention because they comprise a growing proportion of patients and tend to have poor clinical outcomes. The objective of this study was to compare the characteristics and outcomes of immunocompromised and immunocompetent patients with SCAP, and to investigate the risk factors for mortality in these patients.
We conducted retrospective observational cohort study of patients aged ≥18 years admitted to the intensive care unit (ICU) of an academic tertiary hospital with SCAP between January 2017 and December 2019 and compared the clinical characteristics and outcomes of immunocompromised and immunocompetent patients.
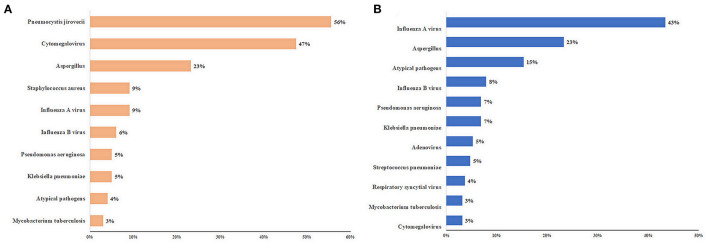
Among the 393 patients, 119 (30.3%) were immunocompromised. Corticosteroid (51.2%) and immunosuppressive drug (23.5%) therapies were the most common causes. Compared to immunocompetent patients, immunocompromised patients had a higher frequency of polymicrobial infection (56.6 vs. 27.5%, < 0.001), early mortality (within 7 days) (26.1 vs. 13.1%, = 0.002), and ICU mortality (49.6 vs. 37.6%, = 0.027). The pathogen distributions differed between immunocompromised and immunocompetent patients. Among immunocompromised patients, and cytomegalovirus were the most common pathogens. Immunocompromised status (OR: 2.043, 95% CI: 1.114-3.748, = 0.021) was an independent risk factor for ICU mortality. Independent risk factors for ICU mortality in immunocompromised patients included age ≥ 65 years (odds ratio [OR]: 9.098, 95% confidence interval [CI]: 1.472-56.234, = 0.018), SOFA score [OR: 1.338, 95% CI: 1.048-1.708, = 0.019), lymphocyte count < 0.8 × 10/L (OR: 6.640, 95% CI: 1.463-30.141, = 0.014), D-dimer level (OR: 1.160, 95% CI: 1.013-1.329, = 0.032), FiO > 0.7 (OR: 10.228, 95% CI: 1.992-52.531, = 0.005), and lactate level (OR: 4.849, 95% CI: 1.701-13.825, = 0.003).
Immunocompromised patients with SCAP have distinct clinical characteristics and risk factors that should be considered in their clinical evaluation and management.
免疫功能低下的重症社区获得性肺炎(SCAP)患者需要特别关注,因为他们在患者中的比例不断增加,且临床结局较差。本研究旨在比较免疫功能低下和免疫功能正常的 SCAP 患者的特征和结局,并探讨这些患者死亡的危险因素。
我们对 2017 年 1 月至 2019 年 12 月期间入住我院 ICU 的年龄≥18 岁的 SCAP 患者进行了回顾性观察性队列研究,并比较了免疫功能低下和免疫功能正常患者的临床特征和结局。
在 393 例患者中,119 例(30.3%)为免疫功能低下。皮质类固醇(51.2%)和免疫抑制药物(23.5%)治疗是最常见的原因。与免疫功能正常的患者相比,免疫功能低下的患者更常发生混合感染(56.6% vs. 27.5%, < 0.001)、早期死亡率(7 天内)(26.1% vs. 13.1%, = 0.002)和 ICU 死亡率(49.6% vs. 37.6%, = 0.027)。免疫功能低下和免疫功能正常患者的病原体分布不同。在免疫功能低下的患者中, 和巨细胞病毒是最常见的病原体。免疫功能低下状态(OR:2.043,95%CI:1.114-3.748, = 0.021)是 ICU 死亡率的独立危险因素。免疫功能低下患者 ICU 死亡率的独立危险因素包括年龄≥65 岁(OR:9.098,95%CI:1.472-56.234, = 0.018)、SOFA 评分(OR:1.338,95%CI:1.048-1.708, = 0.019)、淋巴细胞计数<0.8×10/L(OR:6.640,95%CI:1.463-30.141, = 0.014)、D-二聚体水平(OR:1.160,95%CI:1.013-1.329, = 0.032)、FiO >0.7(OR:10.228,95%CI:1.992-52.531, = 0.005)和乳酸水平(OR:4.849,95%CI:1.701-13.825, = 0.003)。
免疫功能低下的 SCAP 患者具有独特的临床特征和危险因素,在临床评估和管理中应予以考虑。