Pruis Melinda A, Veerman G D Marijn, Hassing H Carlijne, Lanser Daan A C, Paats Marthe S, van Schaik Ron H N, Mathijssen Ron H J, Manintveld Olivier, Dingemans Anne-Marie C
Department of Medical Oncology, Erasmus MC Cancer Institute, University Medical Centre, Rotterdam, the Netherlands.
Department of Pulmonary Medicine, Erasmus MC Cancer Institute, University Medical Centre, Rotterdam, the Netherlands.
JACC CardioOncol. 2023 Jan 17;5(1):102-113. doi: 10.1016/j.jaccao.2022.09.006. eCollection 2023 Feb.
Anaplastic lymphoma kinase (ALK) translocations in metastatic non-small cell lung cancer (3% to 7%) predict for response to ALK-inhibitors (eg, alectinib, first line), resulting in a 5-year survival rate of ∼60% and median progression-free survival of 34.8 months. Although the overall toxicity rate of alectinib is acceptable, unexplained adverse events, including edema and bradycardia, may indicate potential cardiac toxicity.
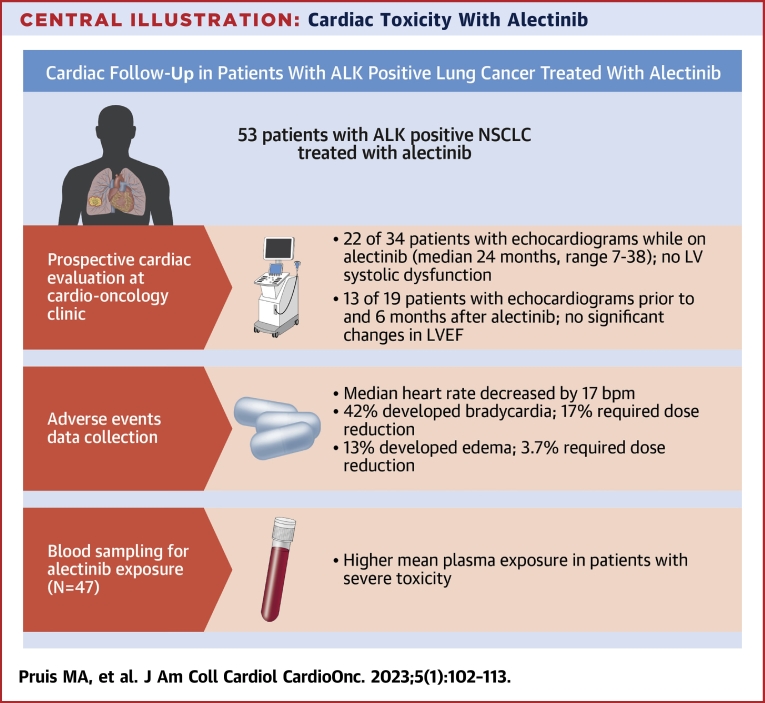
This study's aim was to investigate the cardiotoxicity profile and exposure-toxicity relationship of alectinib.
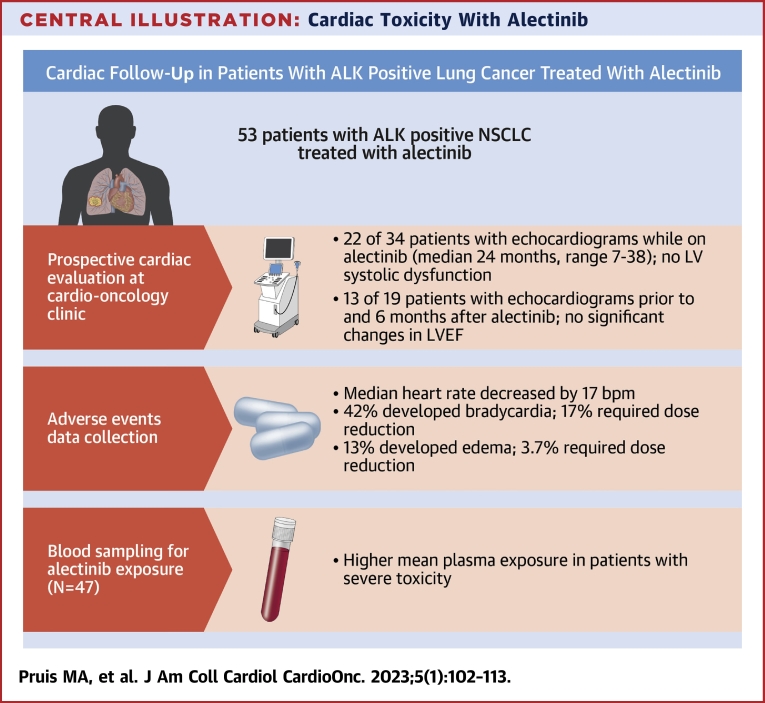
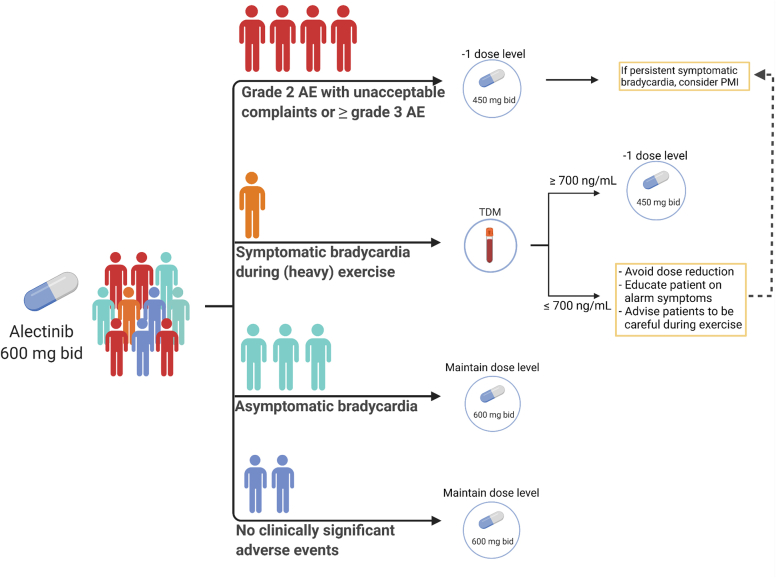
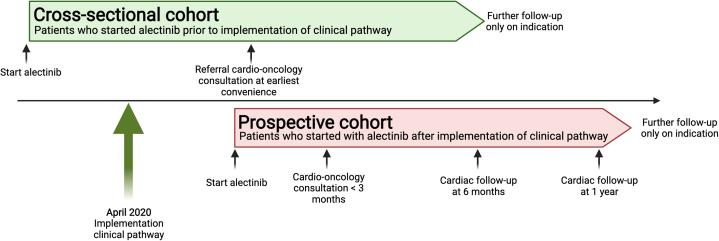
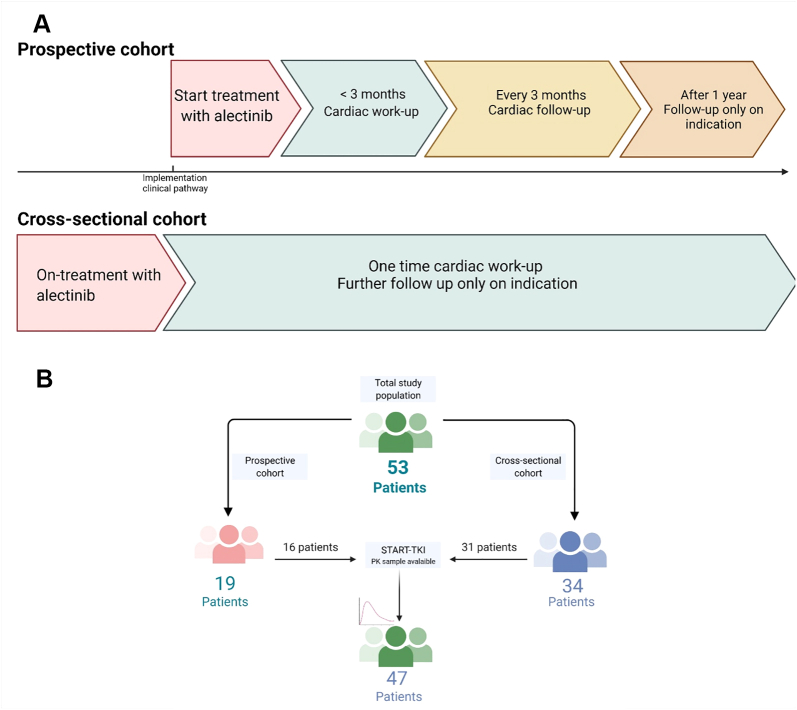
Between April 2020 and September 2021, 53 patients with ALK-positive non-small cell lung cancer treated with alectinib were included. Patients starting with alectinib after April 2020 underwent a cardiac work-up at start, at 6 months and at 1 year at the cardio-oncology outpatients' clinic. Patients already receiving alectinib >6 months underwent 1 cardiac evaluation. Bradycardia, edema, and severe alectinib toxicity (grade ≥3 and grade ≥2 adverse events leading to dose modifications) data were collected. Alectinib steady-state trough concentrations were used for exposure-toxicity analyses.
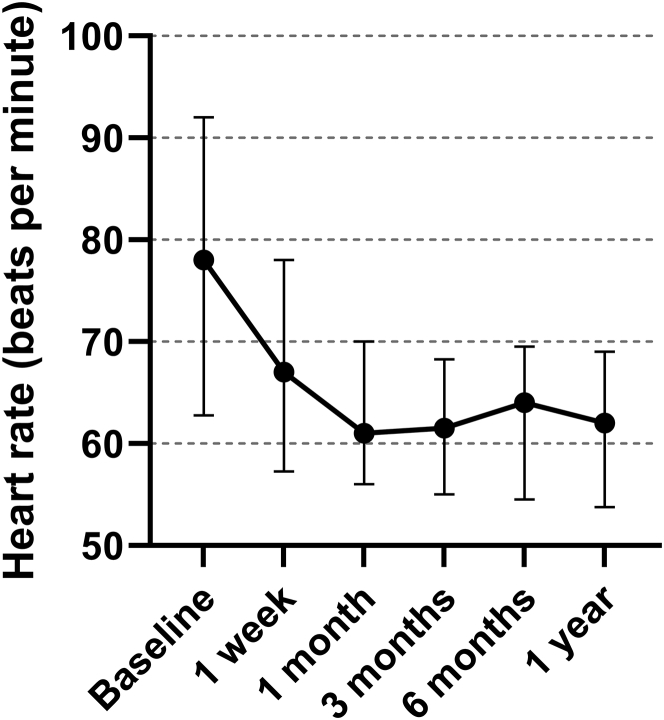
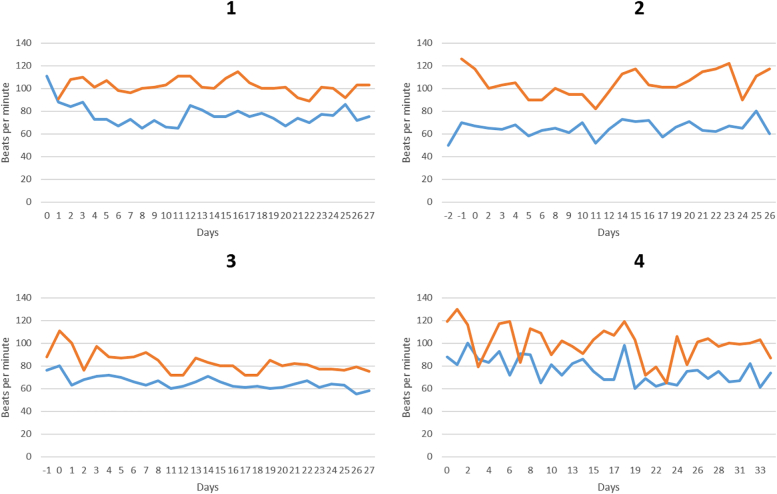
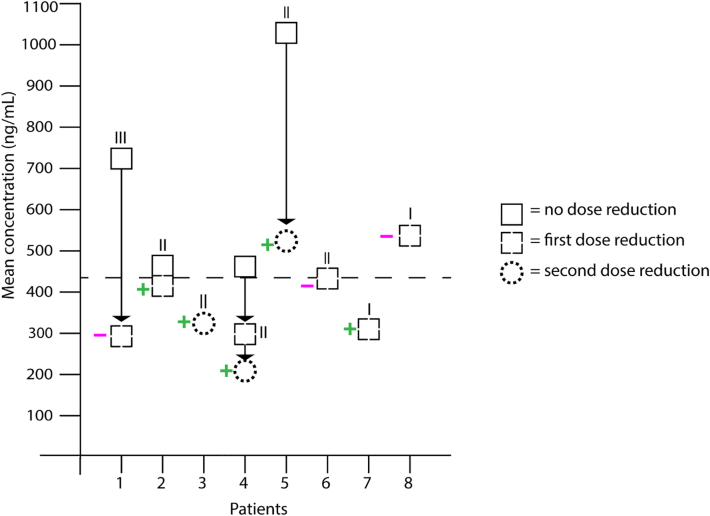
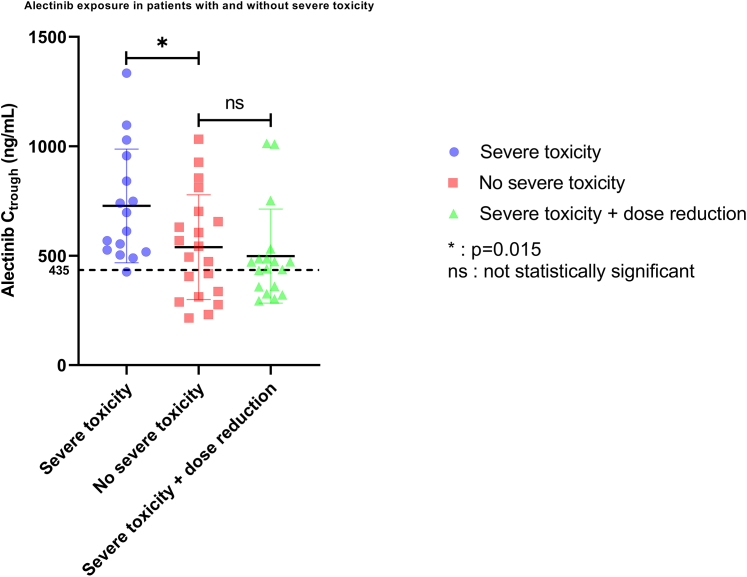
Left ventricular ejection fraction remained stable in all patients who underwent an on-treatment cardiac evaluation (n = 34; median 62%; IQR: 58%-64%). Twenty-two patients (42%) developed alectinib-related bradycardia (6 symptomatic bradycardia). One patient underwent a pacemaker implantation for severe symptomatic bradycardia. Severe toxicity was significantly associated with a 35% higher alectinib mean C (728 vs 539 ng/mL, SD = 83 ng/mL; 1-sided = 0.015).
No patients showed signs of a diminished left ventricular ejection fraction. Alectinib caused more bradycardia than previously reported (42%) with some instances of severe symptomatic bradycardia. Patients with severe toxicity generally had an elevated exposure above the therapeutic threshold.
转移性非小细胞肺癌中间变性淋巴瘤激酶(ALK)易位(3%至7%)预示着对ALK抑制剂(如一线用药阿来替尼)有反应,5年生存率约为60%,无进展生存期的中位数为34.8个月。尽管阿来替尼的总体毒性率可以接受,但包括水肿和心动过缓在内的不明原因不良事件可能表明存在潜在心脏毒性。
本研究旨在调查阿来替尼的心脏毒性特征及暴露-毒性关系。
纳入2020年4月至2021年9月期间接受阿来替尼治疗的53例ALK阳性非小细胞肺癌患者。2020年4月后开始使用阿来替尼的患者在开始治疗时、6个月时和1年时在心脏肿瘤门诊接受心脏检查。已接受阿来替尼治疗超过6个月的患者接受1次心脏评估。收集心动过缓、水肿和严重阿来替尼毒性(≥3级和导致剂量调整的≥2级不良事件)数据。使用阿来替尼稳态谷浓度进行暴露-毒性分析。
所有接受治疗期间心脏评估的患者(n = 34;中位数62%;四分位间距:58%-64%)左心室射血分数保持稳定。22例患者(42%)出现阿来替尼相关心动过缓(6例有症状心动过缓)。1例患者因严重有症状心动过缓接受了起搏器植入。严重毒性与阿来替尼平均Cmax高35%显著相关(728 vs 539 ng/mL,标准差 = 83 ng/mL;单侧P = 0.015)。
没有患者出现左心室射血分数降低的迹象。阿来替尼导致的心动过缓比之前报道的更多(42%),有一些严重有症状心动过缓的病例。严重毒性患者的暴露水平通常高于治疗阈值。