Department of Paediatrics, Division of Paediatric Critical Care Medicine, Beatrix Children's Hospital, University Medical Center Groningen, Groningen, The Netherlands.
Family and Community Health, University of Pennsylvania, Philadelphia, PA.
Pediatr Crit Care Med. 2023 Jun 1;24(6):e272-e281. doi: 10.1097/PCC.0000000000003211. Epub 2023 Mar 6.
To study the hemodynamic consequences of an open-lung high-frequency oscillatory ventilation (HFOV) strategy in patients with an underlying cardiac anomaly with or without intracardiac shunt or primary pulmonary hypertension with severe lung injury.
Secondary analysis of prospectively collected data.
Medical-surgical PICU.
Children less than 18 years old with cardiac anomalies (± intracardiac shunt) or primary pulmonary hypertension.
None.
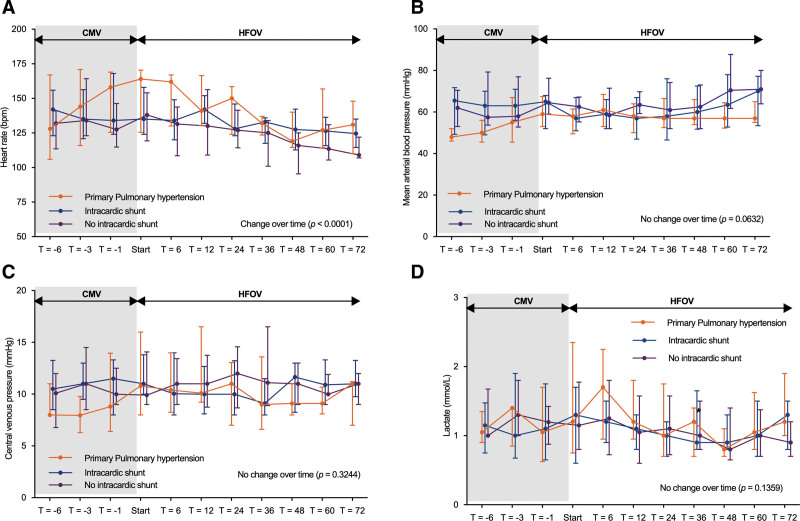
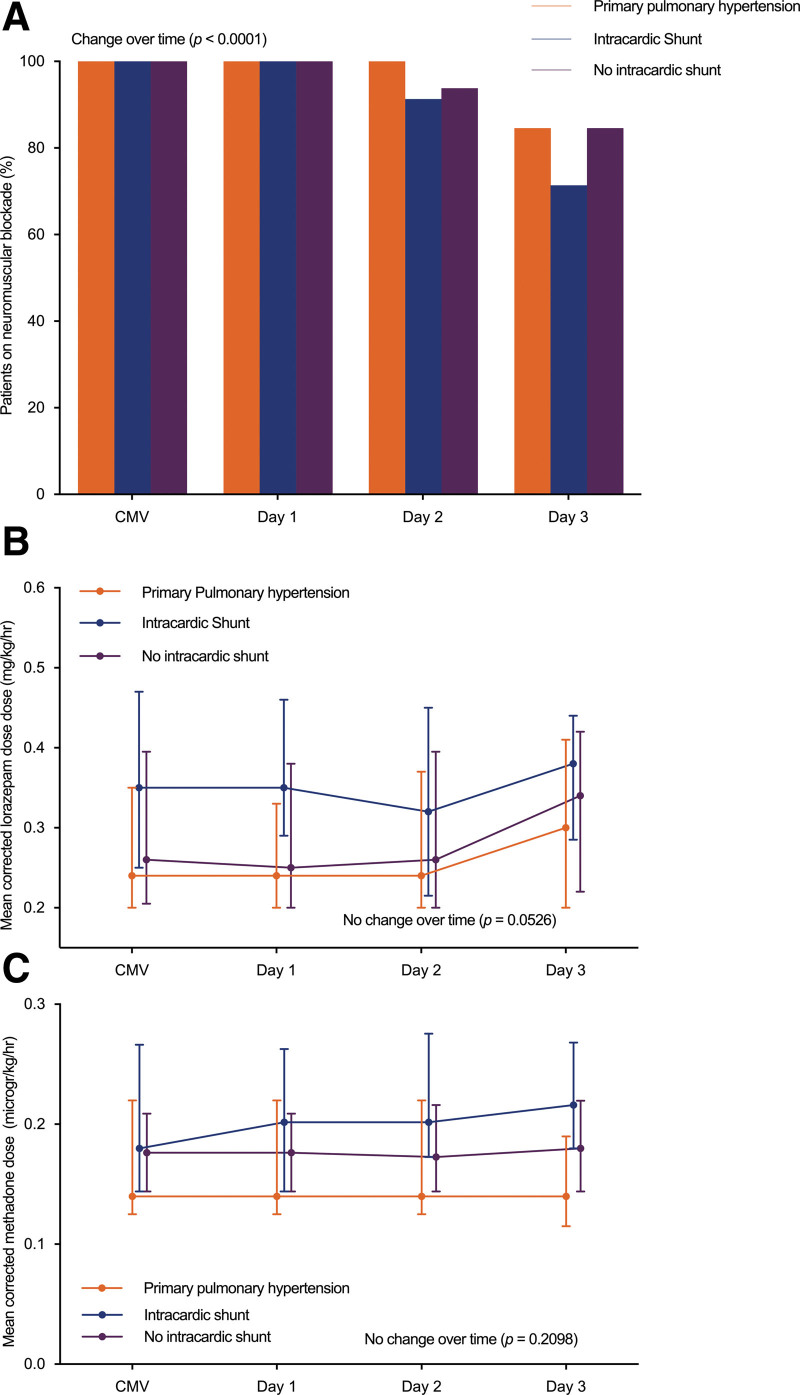
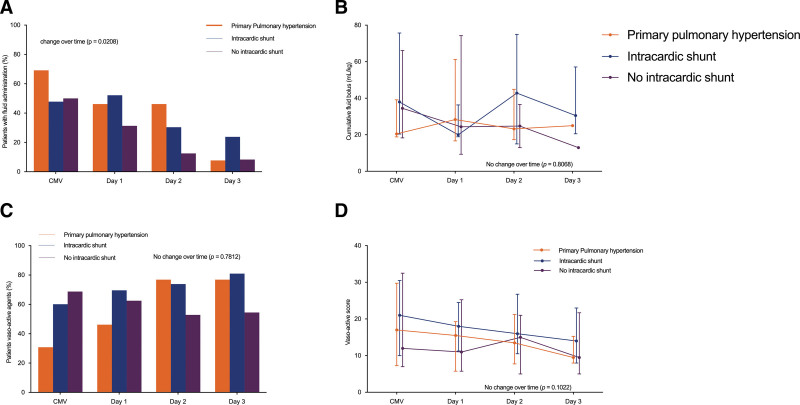
Data from 52 subjects were analyzed, of whom 39 of 52 with cardiac anomaly (23/39 with intracardiac shunt) and 13 of 52 with primary pulmonary hypertension. Fourteen patients were admitted postoperatively, and 26 patients were admitted with acute respiratory failure. Five subjects (9.6%) were canulated for ECMO (of whom four for worsening respiratory status). Ten patients (19.2%) died during PICU stay. Median conventional mechanical ventilation settings prior to HFOV were peak inspiratory pressure 30 cm H 2 O (27-33 cm H 2 O), positive end-expiratory pressure 8 cm H 2 O (6-10 cm H 2 O), and F io2 0.72 (0.56-0.94). After transitioning to HFOV, there was no negative effect on mean arterial blood pressure, central venous pressure, or arterial lactate. Heart rate decreased significantly over time ( p < 0.0001), without group differences. The percentage of subjects receiving a fluid bolus decreased over time ( p = 0.003), especially in those with primary pulmonary hypertension ( p = 0.0155) and without intracardiac shunt ( p = 0.0328). There were no significant differences in the cumulative number of daily boluses over time. Vasoactive Infusion Score did not increase over time. Pa co2 decreased ( p < 0.0002) and arterial pH significantly improved ( p < 0.0001) over time in the whole cohort. Neuromuscular blocking agents were used in all subjects switched to HFOV. Daily cumulative sedative doses were unchanged, and no clinically apparent barotrauma was found.
No negative hemodynamic consequences occurred with an individualized, physiology-based open-lung HFOV approach in patients with cardiac anomalies or primary pulmonary hypertension suffering from severe lung injury.
研究在存在或不存在心内分流或原发性肺动脉高压伴严重肺损伤的基础心脏异常患者中,采用开放式高频振荡通气(HFOV)策略的血流动力学后果。
前瞻性收集数据的二次分析。
内科-外科 PICU。
年龄小于 18 岁的伴有心脏异常(±心内分流)或原发性肺动脉高压的患者。
无。
对 52 名受试者的数据进行了分析,其中 39 名患有心脏异常(23/39 有心内分流),13 名患有原发性肺动脉高压。14 名患者在手术后入住,26 名患者因急性呼吸衰竭入住。5 名患者(9.6%)因 ECMO 插管(其中 4 名因呼吸状态恶化)。10 名患者(19.2%)在 PICU 期间死亡。在开始 HFOV 之前,常规机械通气设置的中位值为吸气峰压 30cmH2O(27-33cmH2O),呼气末正压 8cmH2O(6-10cmH2O),吸入氧浓度 0.72(0.56-0.94)。在过渡到 HFOV 后,平均动脉血压、中心静脉压或动脉血乳酸均无负面影响。心率随时间显著下降(p<0.0001),但无组间差异。接受液体冲击的受试者百分比随时间减少(p=0.003),尤其是在原发性肺动脉高压患者(p=0.0155)和无心内分流患者(p=0.0328)中。随着时间的推移,每日冲击次数的累积量无显著差异。血管活性药物输注评分随时间无显著增加。整个队列的 PaCO2 随时间降低(p<0.0002),动脉 pH 值显著改善(p<0.0001)。所有切换到 HFOV 的患者均使用神经肌肉阻滞剂。每日累积镇静剂量保持不变,未发现明显的气压伤。
在患有严重肺损伤的伴有心脏异常或原发性肺动脉高压的患者中,采用个体化、基于生理学的开放式高频振荡通气方法不会导致血流动力学不良后果。