Clinical Monitoring Research Program Directorate, Frederick National Laboratory for Cancer Research, Frederick, MD.
Rakai Health Sciences Program, Entebbe, Uganda.
J Acquir Immune Defic Syndr. 2023 Jun 1;93(2):143-153. doi: 10.1097/QAI.0000000000003182. Epub 2023 Mar 6.
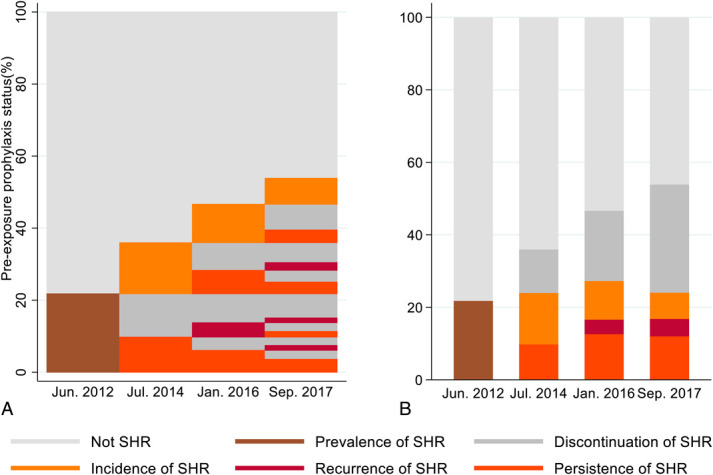
We conducted a retrospective population-based study to describe longitudinal patterns of prevalence, incidence, discontinuation, resumption, and durability of substantial HIV risk behaviors (SHR) for pre-exposure prophylaxis (PrEP) eligibility.
The study was conducted among HIV-negative study participants aged 15-49 years who participated in survey rounds of the Rakai Community Cohort Study between August 2011 and June 2018. Substantial HIV risk was defined based on the Uganda national PrEP eligibility as reporting sexual intercourse with >1 partner of unknown HIV status, nonmarital sex without a condom, having genital ulcers, or having transactional sex. Resumption of SHR meant resuming of SHR after stopping SHR, whereas persistence of SHR meant SHR on >1 consecutive visit. We used generalized estimation equations with log-binomial regression models and robust variance to estimate survey-specific prevalence ratios; Generalized estimation equations with modified Poisson regression models and robust variance to estimate incidence ratios for incidence, discontinuation, and resumption of PrEP eligibility.
Incidence of PrEP eligibility increased from 11.4/100 person-years (pys) in the first intersurvey period to 13.9/100 pys (adjusted incidence rate ratios = 1.28; 95%CI = 1.10-1.30) and declined to 12.6/100 pys (adjusted incidence rate ratios = 1.06; 95%CI = 0.98-1.15) in the second and third intersurvey periods, respectively. Discontinuation rates of SHR for PrEP eligibility were stable (ranging 34.9/100 pys-37.3/100 pys; P = 0.207), whereas resumption reduced from 25.0/100 pys to 14.5/100 pys ( P < 0.001). PrEP eligibility episodes lasted a median time of 20 months (IQR = 10-51).
Pre-exposure prophylaxis use should be tailored to the dynamic nature of PrEP eligibility. Preventive-effective adherence should be adopted for assessment of attrition in PrEP programs.
我们进行了一项基于人群的回顾性研究,旨在描述符合暴露前预防(PrEP)条件的实质性 HIV 风险行为(SHR)的流行率、发生率、停药、恢复和持续时间的纵向变化模式。
该研究纳入了年龄在 15-49 岁之间的 HIV 阴性研究参与者,他们参加了 2011 年 8 月至 2018 年 6 月期间的 Rakai 社区队列研究的调查轮次。实质性 HIV 风险定义为报告与未知 HIV 状况的 >1 名性伴侣发生性行为、无保护措施的非婚姻性行为、生殖器溃疡或交易性性行为。恢复 SHR 意味着停止 SHR 后恢复 SHR,而持续 SHR 意味着连续 >1 次就诊时存在 SHR。我们使用广义估计方程和对数二项式回归模型以及稳健方差来估计特定于调查的流行率比值;使用广义估计方程和修正泊松回归模型以及稳健方差来估计 PrEP 资格的发生率、停药和恢复的发生率比值。
PrEP 资格的发生率从第一个调查间隔期的 11.4/100 人年(pys)增加到 13.9/100 pys(调整后的发病率比 = 1.28;95%CI = 1.10-1.30),并在第二和第三个调查间隔期分别下降至 12.6/100 pys(调整后的发病率比 = 1.06;95%CI = 0.98-1.15)。SHR 停止 PrEP 资格的比例保持稳定(范围为 34.9/100 pys-37.3/100 pys;P = 0.207),而恢复比例从 25.0/100 pys 降至 14.5/100 pys(P < 0.001)。PrEP 资格的持续时间中位数为 20 个月(IQR = 10-51)。
PrEP 的使用应根据 PrEP 资格的动态性质进行调整。应采用预防有效的依从性评估 PrEP 方案中的损耗。