Department of Orthopedic Surgery, Kobe City Medical Center General Hospital 2-1-1 Minamimachi, Minatojima, Chuo-ku, Kobe City, Hyogo prefecture, 650-0047, Japan.
BMC Musculoskelet Disord. 2023 Mar 8;24(1):174. doi: 10.1186/s12891-023-06288-y.
There has been widespread use of short-segment posterior fixation (SSPF) for traumatic thoracolumbar burst fractures. The relationship between the destruction of the vertebral endplate and adjacent disc and postoperative correction loss has been studied in only a few studies. This study investigated the risk factors for correction loss following SSPF.
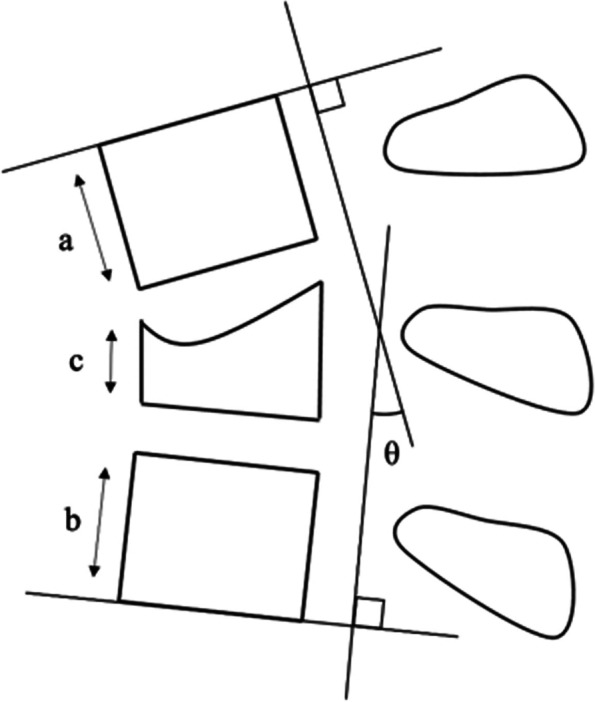
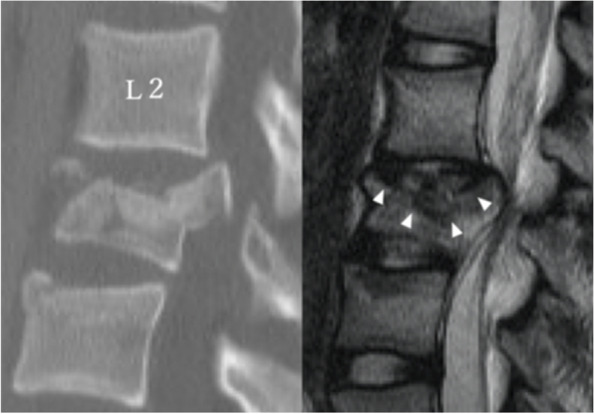
Forty-eight patients (mean age 35.0 years) who underwent SSPF for thoracolumbar burst fractures were enrolled. The mean follow-up period was 25.7 months (12-98 months). The neurological status and postoperative back pain were assessed by the medical records. Segmental kyphotic angle (SKA) and anterior vertebral body height ratio (AVBHR) were measured radiographically to assess indirect vertebral body reduction and local kyphosis. Preoperative Sander's traumatic intervertebral disc lesion (TIDL) classification and AO classification were used to evaluate the severity of disc and vertebral endplate injury. The corrective loss was considered present if ΔSKA was ≥10°. A multivariate logistic regression analysis was performed to identify the risk factors associated with postoperative loss of correction.
The fracture distribution was as follows: 10 at T12, 17 at L1, 10 at L2, 9 at L3, and 2 at L4. Vertebral fractures were classified in the following way: A3 in 13 patients, A4 in 11, B1 in 11, and B2 in 13. In 47 patients (98%), a union of the fractured vertebrae was achieved. SKA and AVBHR improved significantly after surgery from 11.6° to 3.5° and from 67.2 to 90.0%, respectively. However, the correction loss at follow-up was 10.4° and 9.7%, respectively. Twenty patients (42%) had severe TIDL (grade 3). Postoperative ΔSKA and ΔAVBHR were significantly higher in patients with TIDL grade 3 than with TIDL grade 0-2. The presence of cranial TIDL grade 3 and older age were significant risk factors for ΔSKA ≥10° on multivariate logistic regression analysis. All patients could walk at follow-up. TIDL grade 3 and ΔSKA ≥10° were associated with severe postoperative back pain.
Risk factors for loss of correction after SSPF for thoracolumbar burst fractures were severe disc and endplate destruction at the time of injury and older age.
短节段后路固定术(SSPF)已广泛应用于创伤性胸腰椎爆裂性骨折的治疗。仅有少数研究探讨了椎体重建术后椎体终板和相邻椎间盘破坏与矫正丢失之间的关系。本研究旨在探讨 SSPF 术后矫正丢失的相关危险因素。
本研究纳入了 48 例(平均年龄 35.0 岁)接受 SSPF 治疗的胸腰椎爆裂性骨折患者。平均随访时间为 25.7 个月(12-98 个月)。通过病历评估神经功能状态和术后腰痛。影像学上测量节段后凸角(SKA)和椎体前缘高度比(AVBHR),以评估间接椎体复位和局部后凸情况。术前 Sander 外伤性椎间盘损伤(TIDL)分级和 AO 分级用于评估椎间盘和椎体终板损伤的严重程度。如果 ΔSKA≥10°,则认为存在矫正丢失。采用多变量 logistic 回归分析确定与术后矫正丢失相关的危险因素。
骨折分布如下:T12 骨折 10 例,L1 骨折 17 例,L2 骨折 10 例,L3 骨折 9 例,L4 骨折 2 例。椎体骨折分为 A3 型 13 例,A4 型 11 例,B1 型 11 例,B2 型 13 例。47 例(98%)患者骨折椎体获得愈合。术后 SKA 和 AVBHR 分别从 11.6°改善至 3.5°和从 67.2%改善至 90.0%。然而,随访时的矫正丢失分别为 10.4°和 9.7%。20 例(42%)患者存在严重的 TIDL(grade 3)。多变量 logistic 回归分析显示,TIDL grade 3 患者的术后 ΔSKA 和 ΔAVBHR 明显高于 TIDL grade 0-2 患者。颅侧 TIDL grade 3 和年龄较大是 ΔSKA≥10°的显著危险因素。所有患者在随访时均可行走。TIDL grade 3 和 ΔSKA≥10°与严重的术后腰痛相关。
胸腰椎爆裂性骨折患者接受 SSPF 治疗后发生矫正丢失的危险因素为受伤时严重的椎间盘和终板破坏以及年龄较大。