Lindtner Richard A, Mueller Max, Schmid Rene, Spicher Anna, Zegg Michael, Kammerlander Christian, Krappinger Dietmar
Department of Trauma Surgery, Medical University of Innsbruck, Anichstraße 35, 6020, Innsbruck, Austria.
Department of General, Trauma and Reconstructive Surgery, Ludwig Maximilian University Munich, Marchioninistrasse 15, 81377, Munich, Germany.
Arch Orthop Trauma Surg. 2018 Jul;138(7):939-951. doi: 10.1007/s00402-018-2926-9. Epub 2018 Apr 6.
In combined posterior-anterior stabilization of thoracolumbar burst fractures, the expandable vertebral body replacement device (VBRD) is typically placed bisegmentally for anterior column reconstruction (ACR). The aim of this study, however, was to assess feasibility, outcome and potential pitfalls of monosegmental ACR using a VBRD. In addition, clinical and radiological outcome of monosegmental ACR was related to that of bisegmental ACR using the same thoracoscopic technique.
Thirty-seven consecutive neurologically intact patients with burst fractures of the thoracolumbar junction (T11-L2) treated by combined posterior-anterior stabilization were included. Monosegmental ACR was performed in 18 and bisegmental ACR in 19 patients. Fracture type and extent of vertebral body comminution were determined on preoperative CT scans. Monosegmental and bisegmental kyphosis angles were analyzed preoperatively, postoperatively and at final radiological follow-up. Clinical outcome was assessed after a minimum of 2 years (74 ± 45 months; range 24-154; follow-up rate 89.2%) using VAS Spine Score, RMDQ, ODI and WHOQOL-BREF.
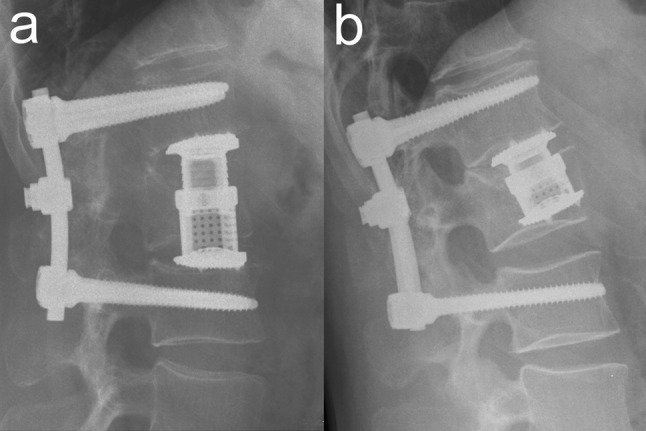
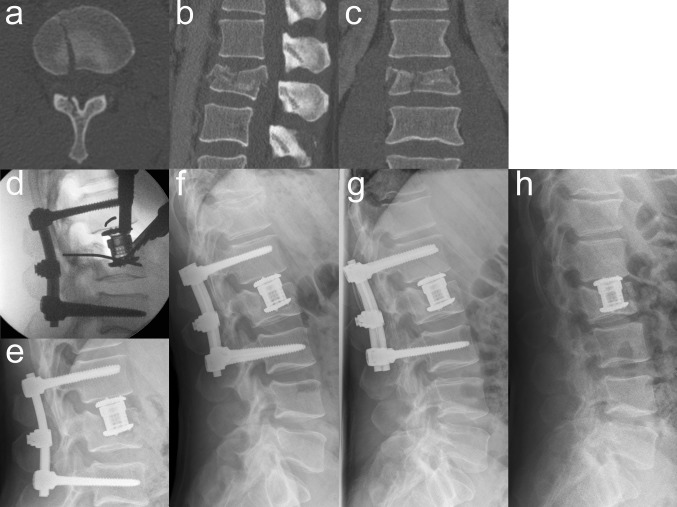
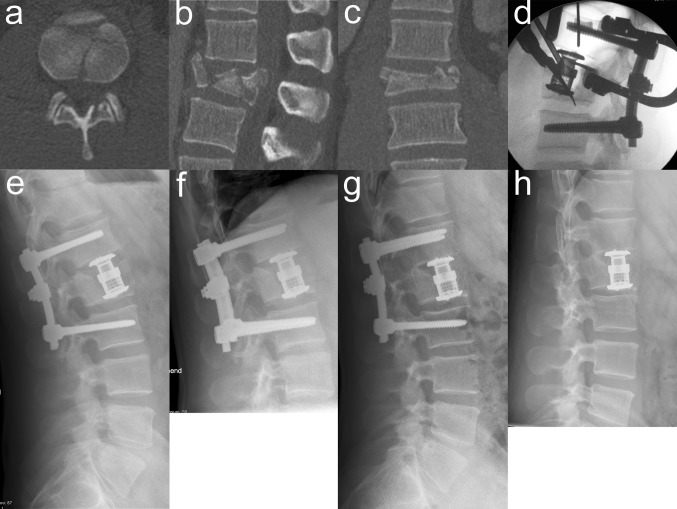
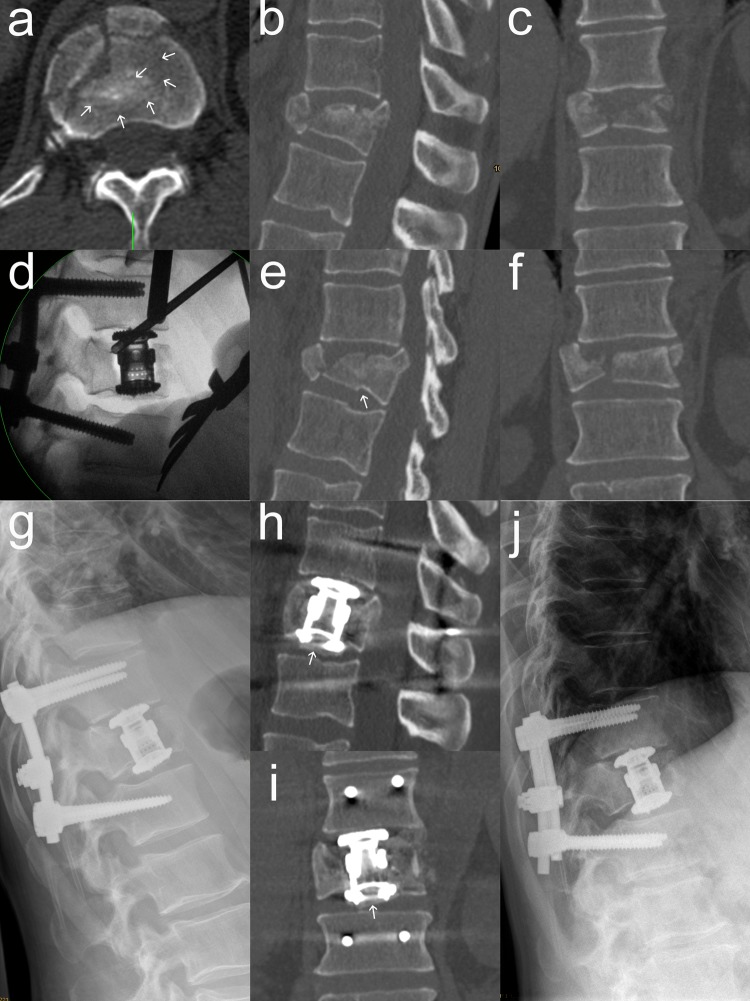
Monosegmental ACR resulted in a mean monosegmental and bisegmental surgical correction of - 15.6 ± 7.7° and - 14.7 ± 8.1°, respectively. Postoperative monosegmental and bisegmental loss of correction averaged 2.7 ± 2.7° and 5.2 ± 3.7°, respectively. Two surgical pitfalls of monosegmental ACR were identified: VBRD positioning (1) onto the weak cancellous bone (too far cranially to the inferior endplate of the fractured vertebra) and (2) onto a significantly compromised inferior endplate with at least two (even subtle) fracture lines. Ignoring these pitfalls resulted in VBRD subsidence in five cases. When relating the clinical and radiological outcome of monosegmental ACR to that of bisegmental ACR, no significant differences were found, except for frequency of VBRD subsidence (5 vs. 0, P = 0.02) and bisegmental loss of correction (5.2 ± 3.7° vs. 2.6 ± 2.5°, P = 0.022). After exclusion of cases with VBRD subsidence, the latter did not reach significance anymore (4.9 ± 4.0° vs. 2.6 ± 2.5°, P = 0.084).
This study indicates that monosegmental ACR using a VBRD is feasible in thoracolumbar burst fractures if the inferior endplate is intact (incomplete burst fractures) or features only a single simple split fracture line (burst-split fractures). If the two identified pitfalls are avoided, monosegmental ACR may be a viable alternative to bisegmental ACR in selected thoracolumbar burst fractures to spare a motion segment and to reduce the distance for bony fusion.
在胸腰椎爆裂骨折的前后联合固定中,可扩张椎体置换装置(VBRD)通常分两节段放置以进行前柱重建(ACR)。然而,本研究的目的是评估使用VBRD进行单节段ACR的可行性、结果及潜在陷阱。此外,单节段ACR的临床和影像学结果与使用相同胸腔镜技术的双节段ACR的结果相关。
纳入37例经前后联合固定治疗的胸腰段交界处(T11-L2)爆裂骨折且神经功能完整的连续患者。18例患者进行单节段ACR,19例患者进行双节段ACR。术前CT扫描确定骨折类型和椎体粉碎程度。术前、术后及最终影像学随访时分析单节段和双节段后凸角。使用脊柱视觉模拟评分(VAS)、罗兰-莫里斯残疾问卷(RMDQ)、Oswestry功能障碍指数(ODI)和世界卫生组织生存质量简表(WHOQOL-BREF)在至少2年(74±45个月;范围24-154个月;随访率89.2%)后评估临床结果。
单节段ACR导致平均单节段和双节段手术矫正分别为-15.6±7.7°和-14.7±8.1°。术后单节段和双节段矫正丢失平均分别为2.7±2.7°和5.2±3.7°。确定了单节段ACR的两个手术陷阱:VBRD定位(1)在薄弱的松质骨上(位于骨折椎体下终板上方太远)和(2)在有至少两条(甚至细微)骨折线的明显受损的下终板上。忽略这些陷阱导致5例VBRD下沉。当将单节段ACR的临床和影像学结果与双节段ACR的结果进行比较时,除了VBRD下沉频率(5例对0例,P=0.02)和双节段矫正丢失(5.2±3.7°对2.6±2.5°,P=0.022)外,未发现显著差异。排除VBRD下沉的病例后,后者不再具有统计学意义(4.9±4.0°对2.6±2.5°,P=0.084)。
本研究表明,如果下终板完整(不完全爆裂骨折)或仅具有一条简单的劈裂骨折线(爆裂-劈裂骨折),则在胸腰椎爆裂骨折中使用VBRD进行单节段ACR是可行的。如果避免两个已确定的陷阱,对于选定的胸腰椎爆裂骨折,单节段ACR可能是双节段ACR的可行替代方案,以保留一个活动节段并减少骨融合的距离。