Cardiology Division, Pisa University Hospital and Chair of Cardiology University of Pisa Italy.
Nuffield Department of Surgical Sciences Oxford University John Radcliffe Hospital Oxford United Kingdom.
J Am Heart Assoc. 2023 Mar 21;12(6):e026943. doi: 10.1161/JAHA.122.026943. Epub 2023 Mar 9.
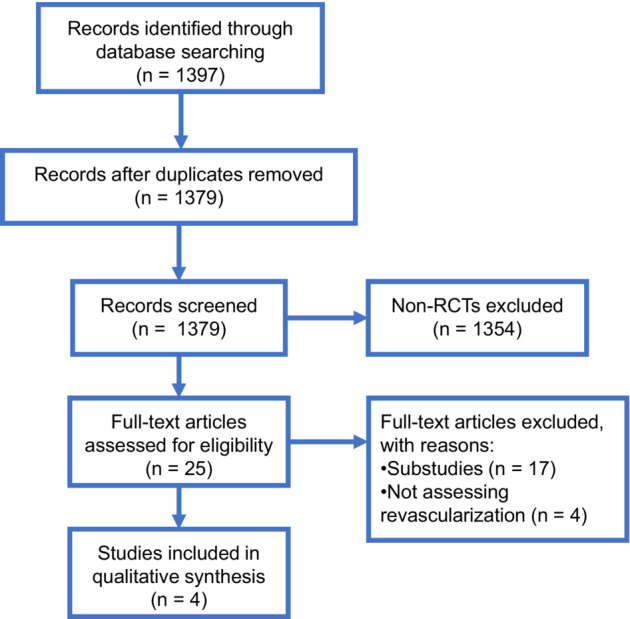
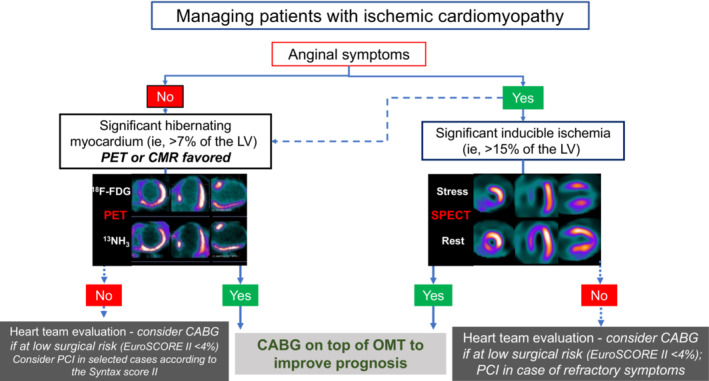
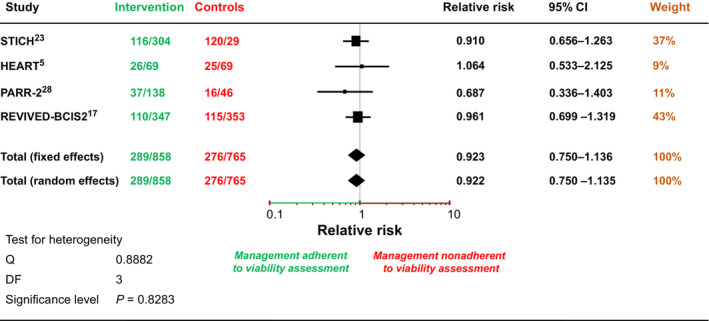
Background Myocardial revascularization has been advocated to improve myocardial function and prognosis in ischemic cardiomyopathy (ICM). We discuss the evidence for revascularization in patients with ICM and the role of ischemia and viability detection in guiding treatment. Methods and Results We searched for randomized controlled trials evaluating the prognostic impact of revascularization in ICM and the value of viability imaging for patient management. Out of 1397 publications, 4 randomized controlled trials were included, enrolling 2480 patients. Three trials (HEART [Heart Failure Revascularisation Trial], STICH [Surgical Treatment for Ischemic Heart Failure], and REVIVED [REVascularization for Ischemic VEntricular Dysfunction]-BCIS2) randomized patients to revascularization or optimal medical therapy. HEART was stopped prematurely without showing any significant difference between treatment strategies. STICH showed a 16% lower mortality with bypass surgery compared with optimal medical therapy at a median follow-up of 9.8 years. However, neither the presence/extent of left ventricle viability nor ischemia interacted with treatment outcomes. REVIVED-BCIS2 showed no difference in the primary end point between percutaneous revascularization or optimal medical therapy. PARR-2 (Positron Emission Tomography and Recovery Following Revascularization) randomized patients to imaging-guided revascularization versus standard care, with neutral results overall. Information regarding the consistency of patient management with viability testing results was available in ≈65% of patients (n=1623). No difference in survival was revealed according to adherence or no adherence to viability imaging. Conclusions In ICM, the largest randomized controlled trial, STICH, suggests that revascularization improves patients' prognosis at long-term follow-up, whereas evidence supports no benefit of percutaneous coronary intervention. Data from randomized controlled trials do not support myocardial ischemia or viability testing for treatment guidance. We propose an algorithm for the workup of patients with ICM considering clinical presentation, imaging results, and surgical risk.
心肌血运重建已被提倡用于改善缺血性心肌病(ICM)患者的心肌功能和预后。我们讨论了 ICM 患者血运重建的证据,以及缺血和存活检测在指导治疗中的作用。
我们搜索了评估血运重建对 ICM 预后影响的随机对照试验,以及存活成像对患者管理的价值。在 1397 篇文献中,纳入了 4 项随机对照试验,共纳入 2480 例患者。其中 3 项试验(HEART [心力衰竭血运重建试验]、STICH [缺血性心力衰竭的外科治疗]和 REVIVED [缺血性心室功能障碍的血运重建]-BCIS2)将患者随机分为血运重建或最佳药物治疗组。HEART 提前终止,两种治疗策略之间没有显示出任何显著差异。STICH 显示与最佳药物治疗相比,旁路手术可使死亡率降低 16%,中位随访 9.8 年后。然而,左心室存活的存在/程度和缺血均未与治疗结果相互作用。REVIVED-BCIS2 显示经皮血运重建与最佳药物治疗之间在主要终点上无差异。PARR-2(正电子发射断层扫描和血运重建后恢复)将患者随机分为影像学指导的血运重建与标准治疗组,总体结果呈中性。关于与存活检测结果一致的患者管理信息可用于约 65%的患者(n=1623)。根据是否遵循或不遵循存活成像,生存无差异。
在 ICM 中,最大的随机对照试验 STICH 表明,长期随访时血运重建可改善患者预后,而数据支持经皮冠状动脉介入治疗无益。随机对照试验的数据不支持心肌缺血或存活检测用于治疗指导。我们提出了一种考虑临床表型、影像学结果和手术风险的 ICM 患者检查方法的算法。