Department of Psychology, University of Arizona, Tucson, Arizona, USA.
Department of Social Sciences and Health Policy, Wake Forest University School of Medicine, Winston-Salem, North Carolina, USA.
Oncology. 2023;101(5):328-342. doi: 10.1159/000528963. Epub 2023 Mar 9.
Smoking after a cancer diagnosis represents a modifiable health risk. It is recommended that oncology clinicians address tobacco use among their patients using the 5As brief model: Asking about use, Advising users to quit, Assessing willingness to quit, Assisting in quit attempts (counseling and medication), and Arranging follow-up. However, cross-sectional studies have found limited adoption of 5As (especially Assist and Arrange) in oncology settings. Further investigation is needed to understand changes in, and factors associated with, 5As delivery over time.
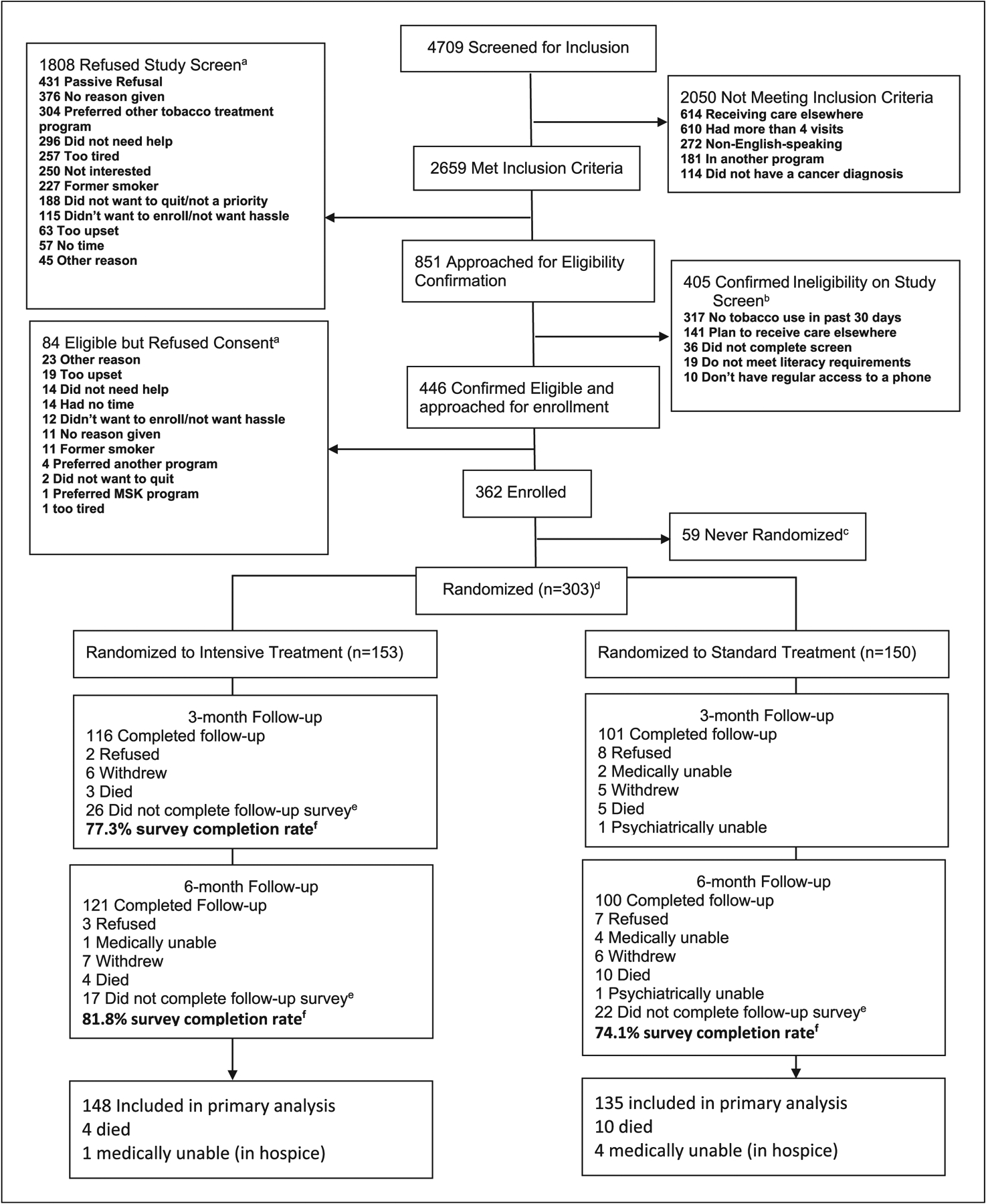
Patients recently diagnosed with cancer and reporting current smoking (N = 303) enrolled in a smoking cessation clinical trial and completed three longitudinal surveys; at pre-intervention baseline and 3- and 6-month follow-up post-enrollment. Patient-level correlates of 5As receipt at baseline, 3 months, and 6 months were identified using multilevel regression models.
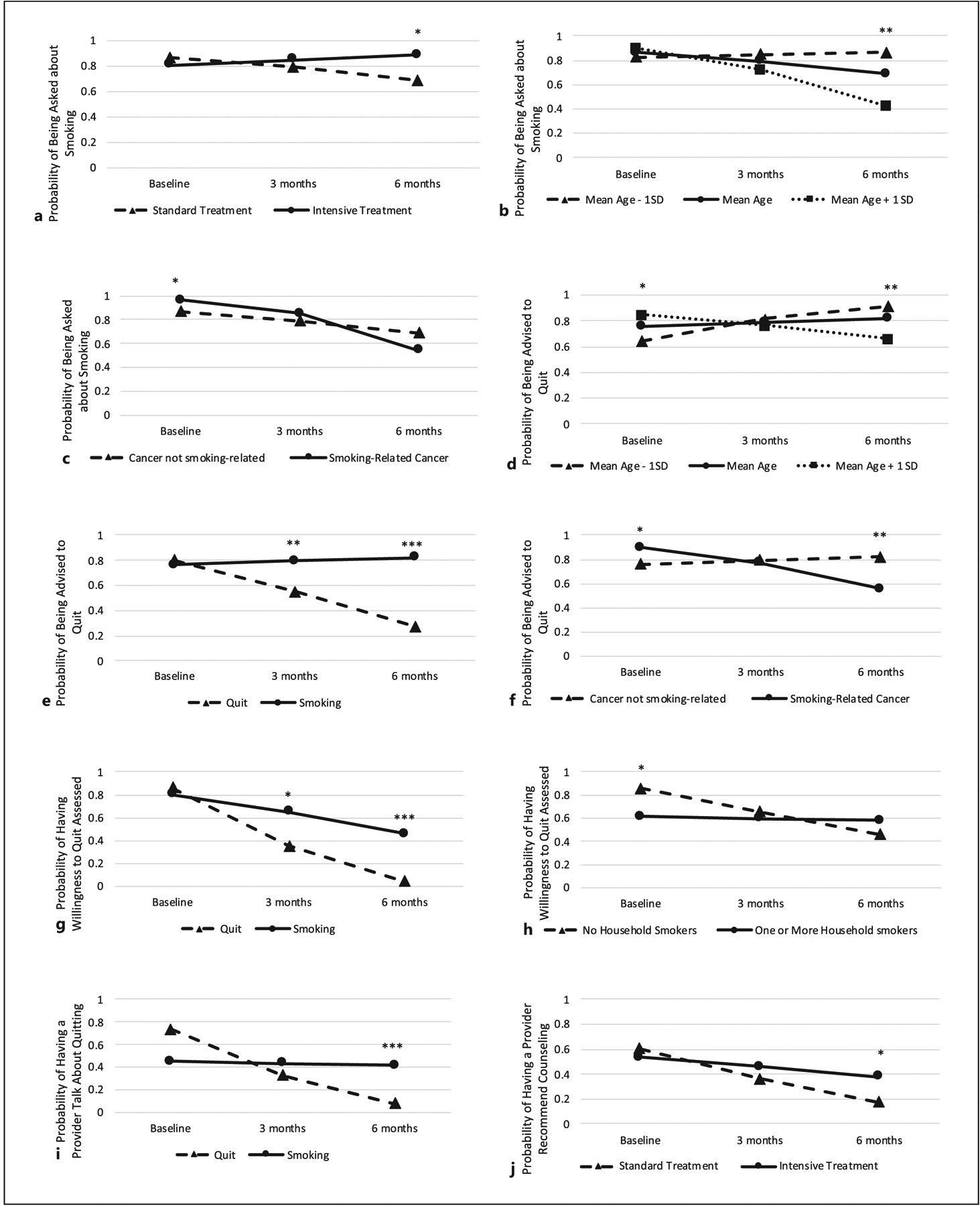
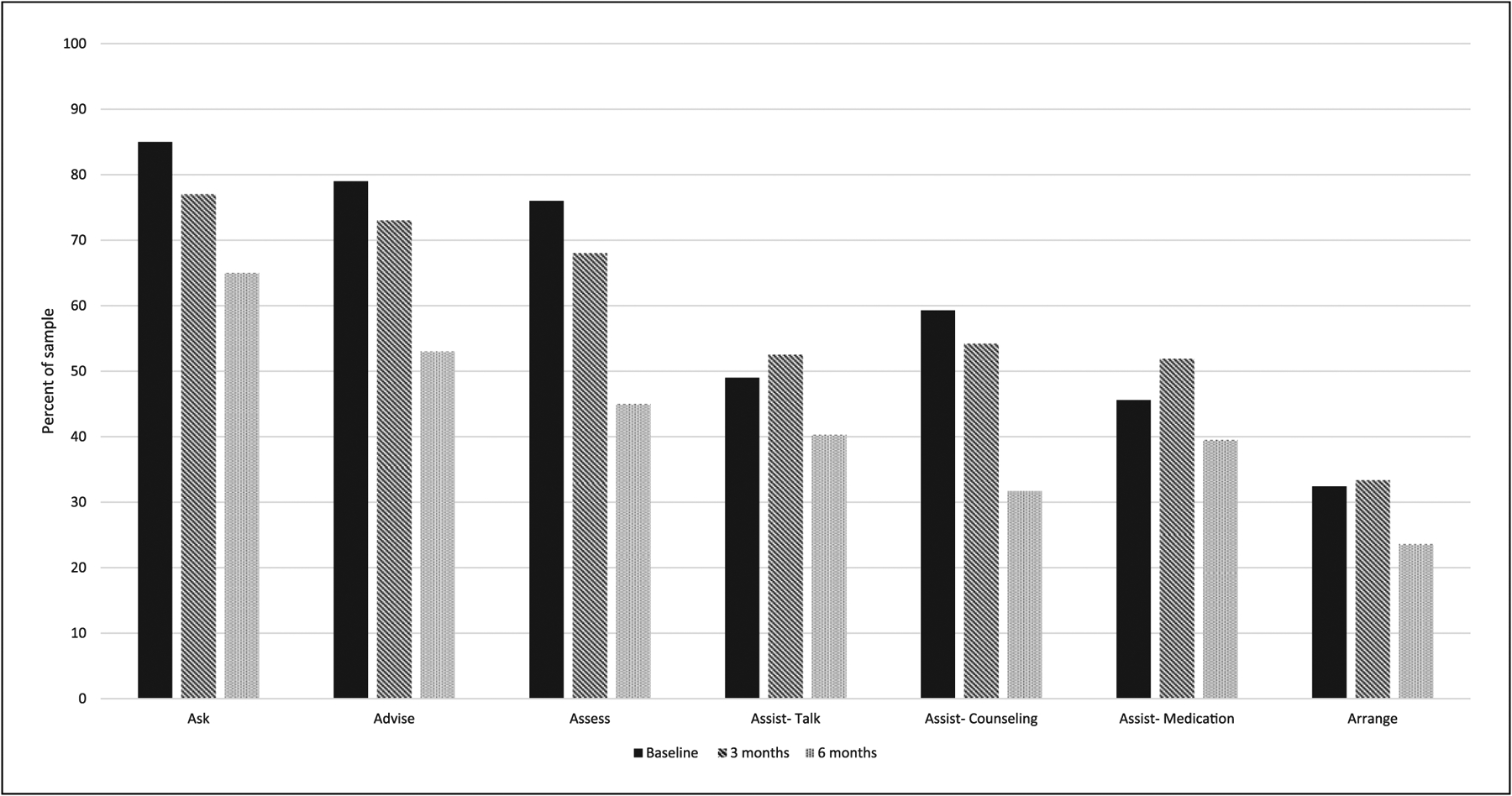
At baseline, patient-reported rates of 5As receipt from oncology clinicians ranged from 85.17% (Ask) to 32.24% (Arrange). Delivery declined from baseline to 6-month follow-up for all 5As, with the largest declines observed for Ask, Advise, Assess, and Assist-Counseling. Diagnosis of a smoking-related cancer was associated with greater odds of 5As receipt at baseline but lower odds at 6-month follow-up. At each time point, female gender, religiosity, advanced disease, cancer-related stigma, and smoking abstinence were associated with lower odds of 5As receipt, while reporting a recent quit attempt prior to enrollment was associated with higher odds of 5As receipt.
Oncology clinicians' 5As delivery declined over time. Clinician delivery of the 5As varied based on patients' sociodemographics, clinical and smoking characteristics, and psychosocial factors.
癌症诊断后吸烟是可改变的健康风险。建议肿瘤临床医生使用 5A 简短模型来解决患者的烟草使用问题:询问使用情况、建议使用者戒烟、评估戒烟意愿、协助戒烟尝试(咨询和药物治疗),以及安排随访。然而,横断面研究发现,5A 在肿瘤学环境中的应用(尤其是协助和安排)有限。需要进一步研究以了解随时间推移 5A 实施的变化和相关因素。
最近被诊断患有癌症且报告目前吸烟的 303 名患者参加了一项戒烟临床试验,并完成了三次纵向调查;在干预前基线和入组后 3 个月和 6 个月随访时进行。使用多层次回归模型确定基线、3 个月和 6 个月时 5A 接收的患者水平相关因素。
基线时,患者报告从肿瘤学临床医生处获得的 5A 率从 85.17%(询问)到 32.24%(安排)不等。所有 5A 的实施均从基线下降到 6 个月随访,其中询问、建议、评估和协助咨询的下降幅度最大。诊断为与吸烟相关的癌症与基线时接受 5A 的几率增加有关,但与 6 个月随访时的几率降低有关。在每个时间点,女性、宗教信仰、晚期疾病、癌症相关耻辱感和吸烟戒断与接受 5A 的几率较低有关,而在入组前报告最近有戒烟尝试与接受 5A 的几率较高有关。
肿瘤临床医生的 5A 实施随时间推移而下降。临床医生提供 5A 的情况因患者的社会人口统计学、临床和吸烟特征以及心理社会因素而异。