Department of Anesthesiology and Intensive Care Medicine, Second Faculty of Medicine, Charles University and University Hospital Motol, Prague, Czech Republic.
Prague Lung Transplant Program, 3rd Department of Surgery, First Faculty of Medicine, Charles University and University Hospital Motol, Prague, Czech Republic.
BMC Pulm Med. 2023 Mar 9;23(1):80. doi: 10.1186/s12890-023-02372-0.
Primary graft dysfunction (PGD) after lung transplantation (LuTx) contributes substantially to early postoperative morbidity. Both intraoperative transfusion of a large amount of blood products during the surgery and ischemia-reperfusion injury after allograft implantation play an important role in subsequent PGD development.
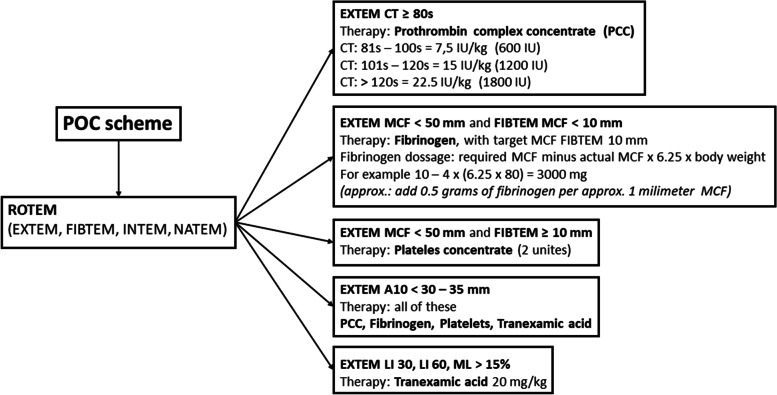
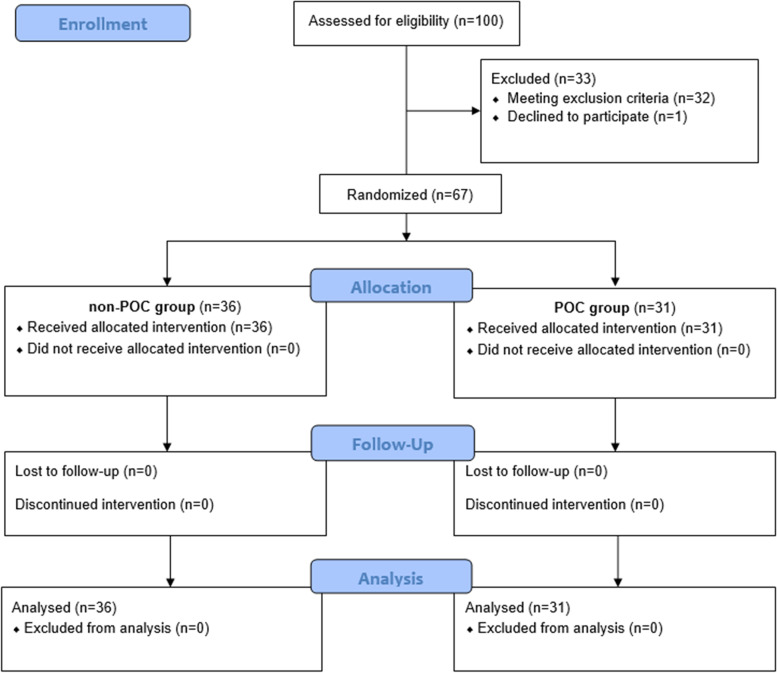
We have previously reported a randomized clinical trial of 67 patients where point of care (POC) targeted coagulopathy management and intraoperative administration of 5% albumin led to significant reduction of blood loss and blood product consumption during the lung transplantation surgery. A secondary analysis of the randomized clinical trial evaluating the effect of targeted coagulopathy management and intraoperative administration of 5% albumin on early lung allograft function after LuTx and 1-year survival was performed.
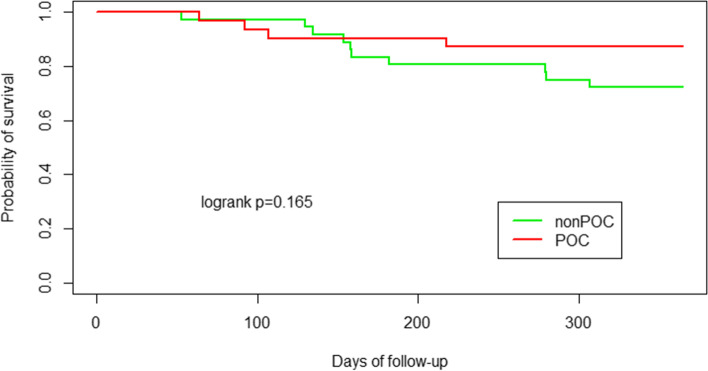
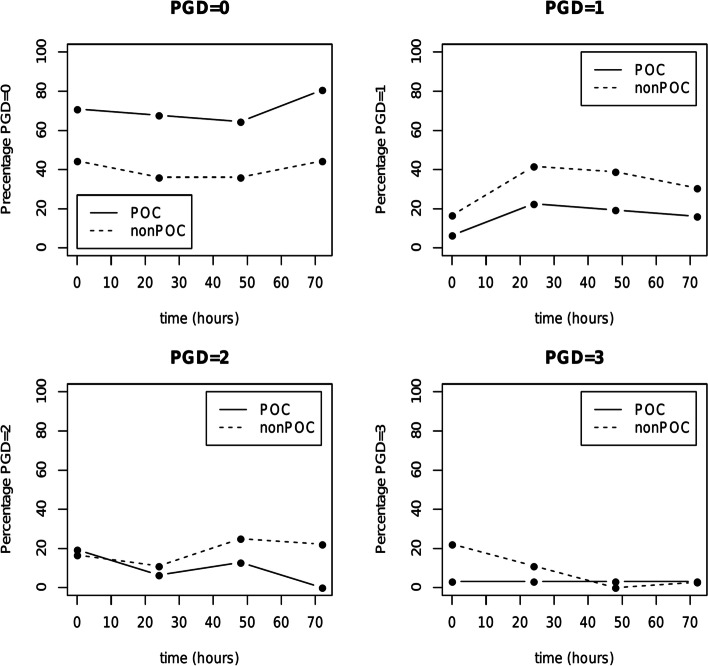
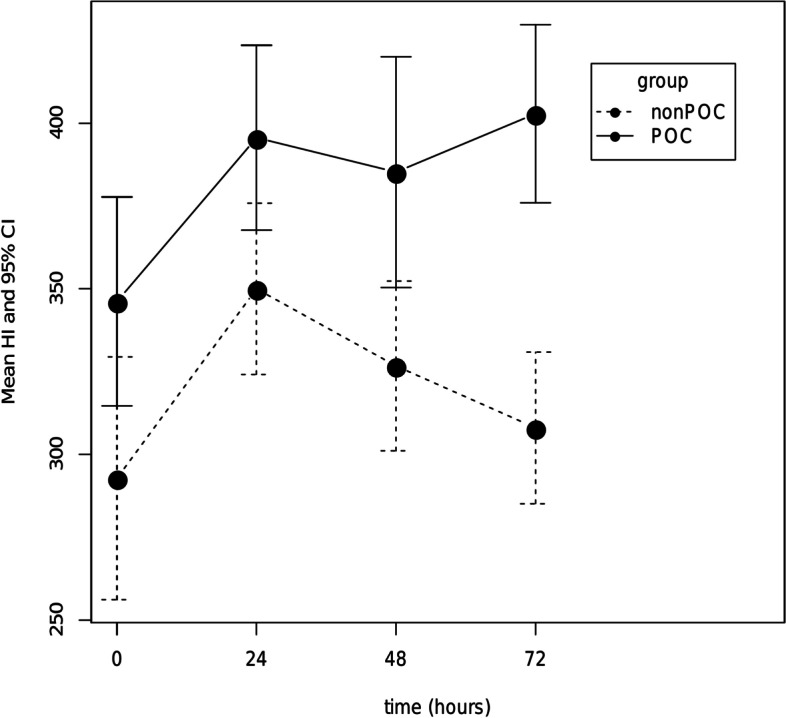
Compared to the patients in the control (non-POC) group, those in study (POC) group showed significantly superior graft function, represented by the Horowitz index (at 72 h after transplantation 402.87 vs 308.03 with p < 0.001, difference between means: 94.84, 95% CI: 60.18-129.51). Furthermore, the maximum doses of norepinephrine administered during first 24 h were significantly lower in the POC group (0.193 vs 0.379 with p < 0.001, difference between the means: 0.186, 95% CI: 0.105-0.267). After dichotomization of PGD (0-1 vs 2-3), significant difference between the non-POC and POC group occurred only at time point 72, when PGD grade 2-3 developed in 25% (n = 9) and 3.2% (n = 1), respectively (p = 0.003). The difference in 1-year survival was not statistically significant (10 patients died in non-POC group vs. 4 patients died in POC group; p = 0.17).
Utilization of a POC targeted coagulopathy management combined with Albumin 5% as primary resuscitative fluid may improve early lung allograft function, provide better circulatory stability during the early post-operative period, and have potential to decrease the incidence of PGD without negative effect on 1-year survival.
This clinical trial was registered at ClinicalTrials.gov (NCT03598907).
肺移植(LuTx)后原发性移植物功能障碍(PGD)是导致早期术后发病率高的主要原因。术中大量输血和同种异体移植后缺血再灌注损伤在随后的 PGD 发展中都起着重要作用。
我们之前报告了一项 67 例患者的随机临床试验,其中采用即时检测(POC)目标凝血障碍管理和术中给予 5%白蛋白,可显著减少肺移植手术中的失血和血液制品的消耗。对该随机临床试验进行了二次分析,以评估 POC 目标凝血障碍管理和术中给予 5%白蛋白对 LuTx 后早期肺移植物功能和 1 年生存率的影响。
与对照组(非 POC)患者相比,研究组(POC)患者的移植物功能明显更好,以霍洛威指数(移植后 72 小时分别为 402.87 和 308.03,p<0.001,差值:94.84,95%置信区间:60.18-129.51)表示。此外,在第 1 天至第 24 小时内给予去甲肾上腺素的最大剂量在 POC 组中明显较低(分别为 0.193 和 0.379,p<0.001,差值:0.186,95%置信区间:0.105-0.267)。PGD(0-1 级对 2-3 级)二分类后,非 POC 组和 POC 组仅在 72 小时时出现显著差异,PGD 2-3 级分别发生在 25%(n=9)和 3.2%(n=1)患者中(p=0.003)。1 年生存率的差异无统计学意义(非 POC 组 10 例患者死亡,POC 组 4 例患者死亡;p=0.17)。
利用即时检测目标凝血障碍管理联合 5%白蛋白作为主要复苏液可能改善早期肺移植物功能,在术后早期提供更好的循环稳定性,并有可能降低 PGD 的发生率,而对 1 年生存率无不利影响。
本临床试验在 ClinicalTrials.gov 注册(NCT03598907)。