Yue Xiaoning, He Xiaoyu, He Shuaijie, Wu Jingjing, Fan Wei, Zhang Haijun, Wang Chengwei
Department of CT&MRI, The First Affiliated Hospital of Medical College, Shihezi University, Shihezi, China.
Department of Pathology, The First Affiliated Hospital of Medical College, Shihezi University, Shihezi, China.
Front Oncol. 2023 Feb 21;13:1081134. doi: 10.3389/fonc.2023.1081134. eCollection 2023.
Tumor grade is associated with the treatment and prognosis of endometrial cancer (EC). The accurate preoperative prediction of the tumor grade is essential for EC risk stratification. Herein, we aimed to assess the performance of a multiparametric magnetic resonance imaging (MRI)-based radiomics nomogram for predicting high-grade EC.
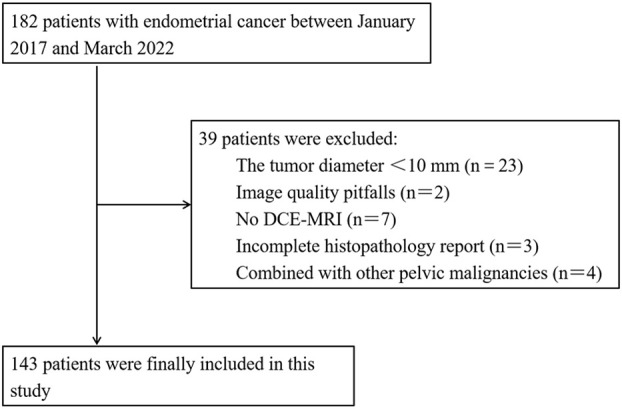
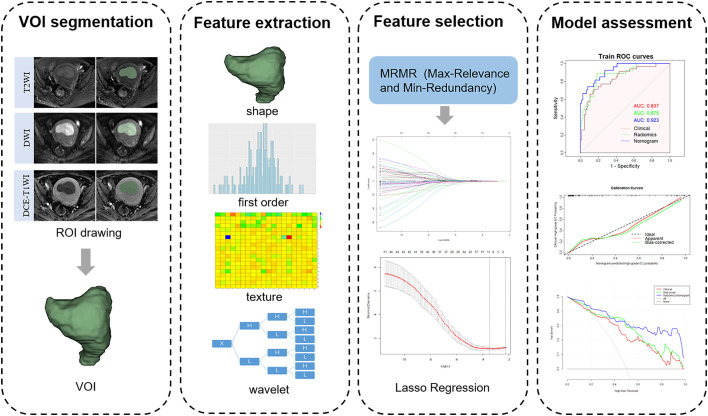
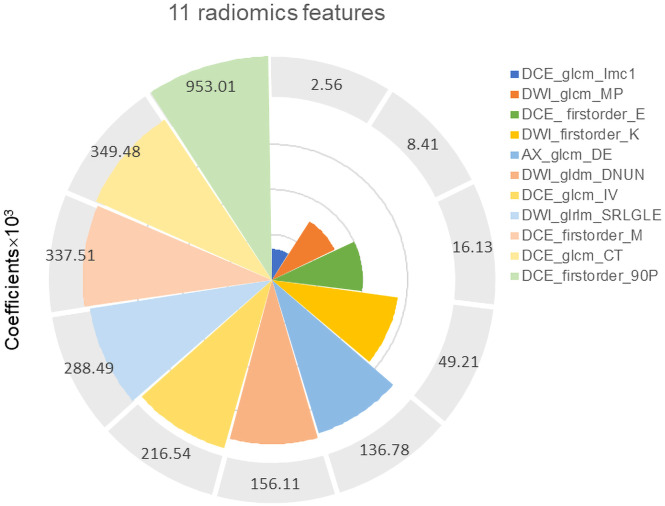
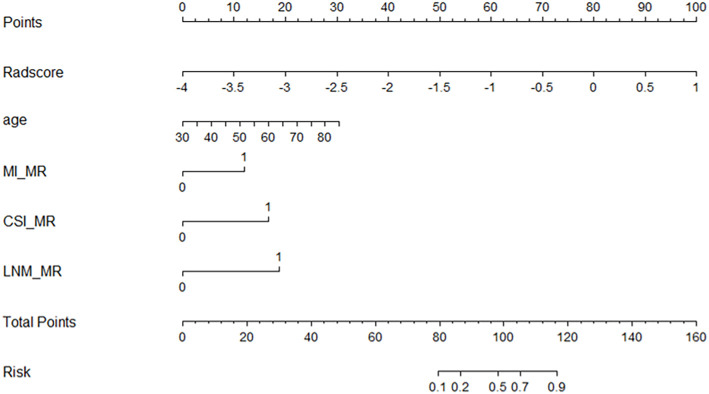
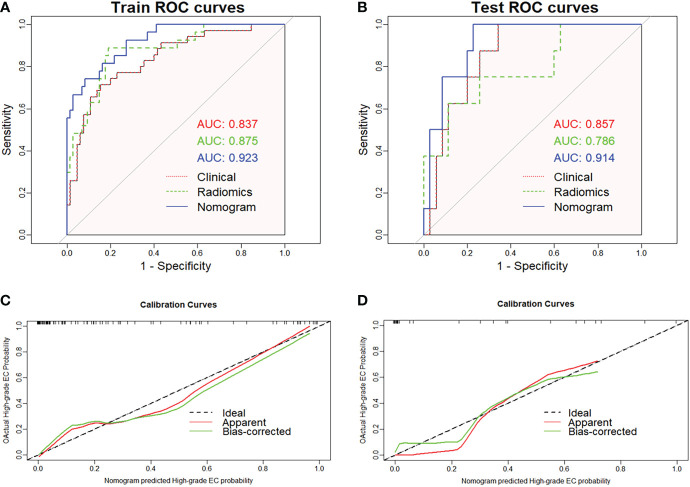
One hundred and forty-three patients with EC who had undergone preoperative pelvic MRI were retrospectively enrolled and divided into a training set ( =100) and a validation set ( =43). Radiomic features were extracted based on T2-weighted, diffusion-weighted, and dynamic contrast-enhanced T1-weighted images. The minimum absolute contraction selection operator (LASSO) was implemented to obtain optimal radiomics features and build the rad-score. Multivariate logistic regression analysis was used to determine the clinical MRI features and build a clinical model. We developed a radiomics nomogram by combining important clinical MRI features and rad-score. A receiver operating characteristic (ROC) curve was used to evaluate the performance of the three models. The clinical net benefit of the nomogram was assessed using decision curve analysis (DCA), net reclassification index (NRI), and integrated discrimination index (IDI).
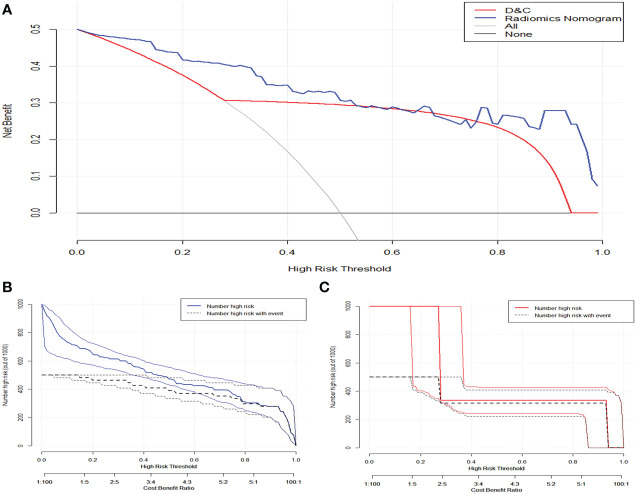
In total, 35/143 patients had high-grade EC and 108 had low-grade EC. The areas under the ROC curves of the clinical model, rad-score, and radiomics nomogram were 0.837 (95% confidence interval [CI]: 0.754-0.920), 0.875 (95% CI: 0.797-0.952), and 0.923 (95% CI: 0.869-0.977) for the training set; 0.857 (95% CI: 0.741-0.973), 0.785 (95% CI: 0.592-0.979), and 0.914 (95% CI: 0.827-0.996) for the validation set, respectively. The radiomics nomogram showed a good net benefit according to the DCA. NRIs were 0.637 (0.214-1.061) and 0.657 (0.079-1.394), and IDIs were 0.115 (0.077-0.306) and 0.053 (0.027-0.357) in the training set and validation set, respectively.
The radiomics nomogram based on multiparametric MRI can predict the tumor grade of EC before surgery and yield a higher performance than that of dilation and curettage.
肿瘤分级与子宫内膜癌(EC)的治疗及预后相关。术前准确预测肿瘤分级对于EC风险分层至关重要。在此,我们旨在评估基于多参数磁共振成像(MRI)的影像组学列线图预测高级别EC的性能。
回顾性纳入143例术前行盆腔MRI检查的EC患者,并分为训练集(n = 100)和验证集(n = 43)。基于T2加权、扩散加权和动态对比增强T1加权图像提取影像组学特征。采用最小绝对收缩选择算子(LASSO)获取最佳影像组学特征并构建影像组学评分(rad-score)。多因素逻辑回归分析用于确定临床MRI特征并构建临床模型。我们通过结合重要的临床MRI特征和rad-score开发了影像组学列线图。采用受试者工作特征(ROC)曲线评估这三种模型的性能。使用决策曲线分析(DCA)、净重新分类指数(NRI)和综合判别指数(IDI)评估列线图的临床净效益。
143例患者中,35例为高级别EC,108例为低级别EC。训练集的临床模型、rad-score和影像组学列线图的ROC曲线下面积分别为0.837(95%置信区间[CI]:0.754 - 0.920)、0.875(95%CI:0.797 - 0.952)和0.923(95%CI:0.869 - 0.977);验证集分别为0.857(95%CI:0.741 - 0.973)、0.785(95%CI:0.592 - 0.979)和0.914(95%CI:0.827 - 0.996)。根据DCA,影像组学列线图显示出良好的净效益。训练集和验证集的NRI分别为0.637(0.214 - 1.061)和0.657(0.079 - 1.394),IDI分别为0.115(0.077 - 0.306)和0.053(0.027 - 0.357)。
基于多参数MRI的影像组学列线图可在术前预测EC的肿瘤分级,且性能优于刮宫术。