Translational and Clinical Research Institute, Newcastle University, Newcastle Upon Tyne, UK.
Nuclear Medicine Department, Newcastle Upon Tyne Hospitals NHS Foundation Trust, Newcastle Upon Tyne, UK.
Eur J Neurol. 2023 Jun;30(6):1585-1593. doi: 10.1111/ene.15783. Epub 2023 Mar 21.
Mild cognitive impairment with Lewy bodies (MCI-LB) is associated with a range of cognitive, motor, neuropsychiatric, sleep, autonomic, and visual symptoms. We investigated the cumulative frequency of symptoms in a longitudinal cohort of MCI-LB compared with MCI due to Alzheimer disease (MCI-AD) and analysed the ability of a previously described 10-point symptom scale to differentiate MCI-LB and MCI-AD, in an independent cohort.
Participants with probable MCI-LB (n = 70), MCI-AD (n = 51), and controls (n = 34) had a detailed clinical assessment and annual follow-up (mean duration = 1.7 years). The presence of a range of symptoms was ascertained using a modified version of the Lewy Body Disease Association Comprehensive LBD Symptom Checklist at baseline assessment and then annually.
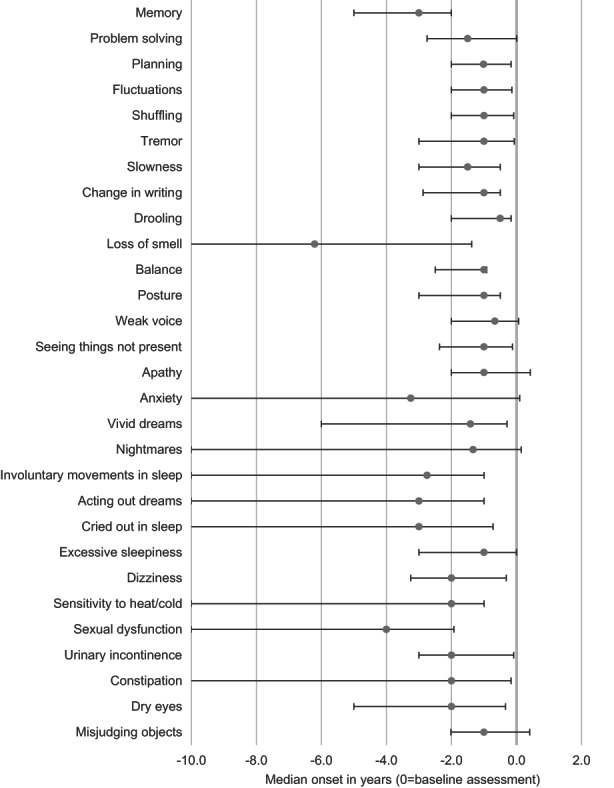
MCI-LB participants experienced a greater mean number of symptoms (24.2, SD = 7.6) compared with MCI-AD (11.3, SD = 7.4) and controls (4.2, SD = 3.1; p < 0.001 for all comparisons). A range of cognitive, parkinsonian, neuropsychiatric, sleep, and autonomic symptoms were significantly more common in MCI-LB than MCI-AD, although when present, the time of onset was similar between the two groups. A previously defined 10-point symptom scale demonstrated very good discrimination between MCI-LB and MCI-AD (area under the receiver operating characteristic curve = 0.91, 95% confidence interval = 0.84-0.98), replicating our previous finding in a new cohort.
MCI-LB is associated with the frequent presence of a particular profile of symptoms compared to MCI-AD. Clinicians should look for evidence of these symptoms in MCI and be aware of the potential for treatment. The presence of these symptoms may help to discriminate MCI-LB from MCI-AD.
路易体轻度认知障碍(MCI-LB)与一系列认知、运动、神经精神、睡眠、自主和视觉症状相关。我们在一个 MCI-LB 的纵向队列中研究了症状的累积频率,与 MCI 归因于阿尔茨海默病(MCI-AD)进行了比较,并在一个独立的队列中分析了先前描述的 10 分症状量表区分 MCI-LB 和 MCI-AD 的能力。
有明确的可能 MCI-LB(n=70)、MCI-AD(n=51)和对照组(n=34)的参与者接受了详细的临床评估和年度随访(平均随访时间为 1.7 年)。在基线评估时以及随后每年使用改良版路易体病协会综合路易体病症状检查表确定各种症状的存在。
与 MCI-AD(11.3,标准差[SD]=7.4)和对照组(4.2,SD=3.1)相比,MCI-LB 参与者的平均症状数量更多(24.2,SD=7.6;所有比较均 p<0.001)。在 MCI-LB 中,一系列认知、帕金森、神经精神、睡眠和自主症状比 MCI-AD 更为常见,尽管在出现这些症状时,两组的发病时间相似。之前定义的 10 分症状量表在 MCI-LB 和 MCI-AD 之间具有非常好的区分能力(接受者操作特征曲线下面积=0.91,95%置信区间=0.84-0.98),在新队列中复制了我们之前的发现。
与 MCI-AD 相比,MCI-LB 常伴有特定的症状谱。临床医生应在 MCI 中寻找这些症状的证据,并意识到治疗的潜力。这些症状的存在可能有助于区分 MCI-LB 和 MCI-AD。