Department of Anesthesiology and Pain Medicine, Chungnam National University Hospital.
Departments of Anesthesiology and Pain Medicine, College of Medicine, Chungnam National University.
Int J Surg. 2023 Jun 1;109(6):1728-1741. doi: 10.1097/JS9.0000000000000270.
Various regional analgesia techniques are used to reduce postoperative pain in patients undergoing lumbar spine surgery. Traditionally, wound infiltration (WI) with local anesthetics has been widely used by surgeons. Recently, other regional analgesia techniques, such as the erector spinae plane block (ESPB) and thoracolumbar interfascial plane (TLIP) block, are being used for multimodal analgesia. The authors aimed to determine the relative efficacy of these using a network meta-analysis.
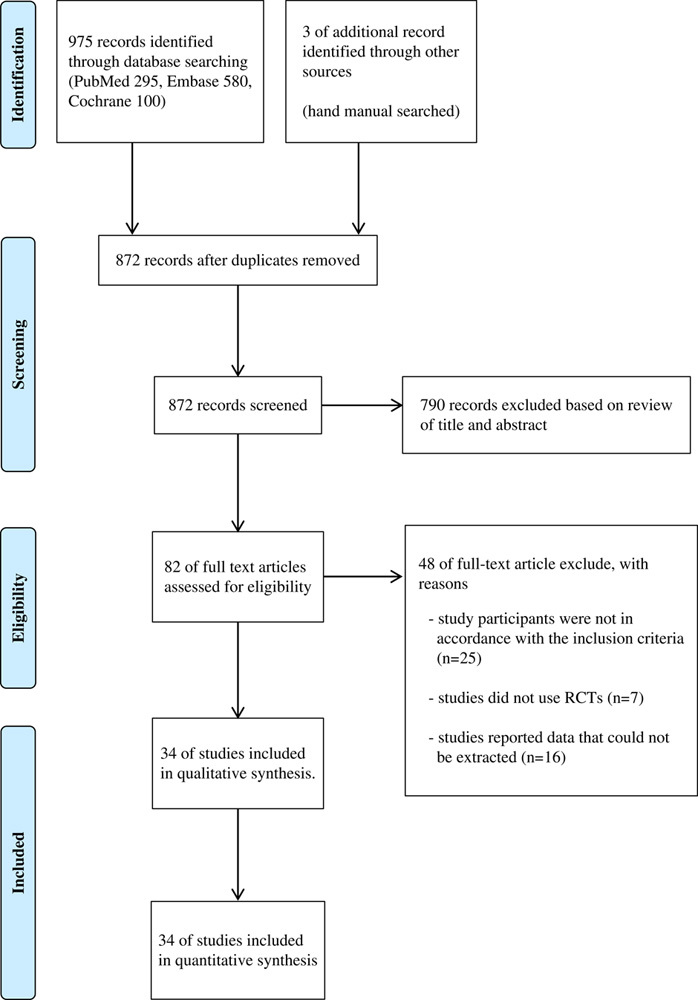
The authors searched PubMed, EMBASE, the Cochrane Controlled Library, and Google Scholar databases to identify all randomized controlled trials that compared the analgesic efficacy of the following interventions: ESPB, TLIP block, WI technique, and controls. The primary endpoint was postoperative opioid consumption during the first 24 hours after surgery, while the pain score, estimated postoperatively at three different time periods, was the secondary objective.
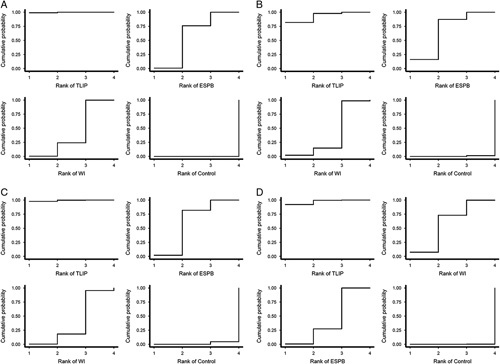
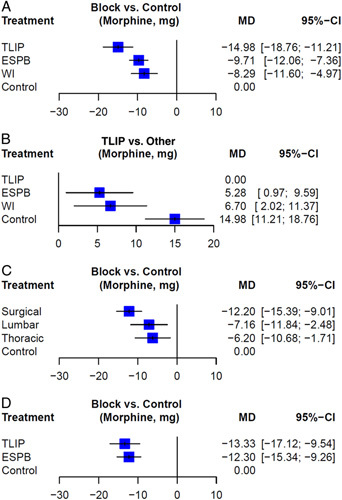
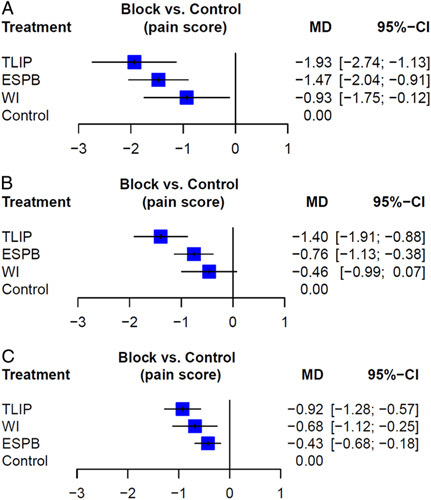
The authors included 34 randomized controlled trials with data from 2365 patients. TLIP showed the greatest reduction in opioid consumption compared to controls [mean difference (MD) =-15.0 mg; 95% CI: -18.8 to -11.2]. In pain scores, TLIP had the greatest effect during all time periods compared to controls (MD=-1.9 in early, -1.4 in middle, -0.9 in late). The injection level of ESPB was different in each study. When only surgical site injection of ESPB was included in the network meta-analysis, there was no difference compared with TLIP (MD=1.0 mg; 95% CI: -3.6 to 5.6).
TLIP showed the greatest analgesic efficacy after lumbar spine surgery, in terms of postoperative opioid consumption and pain scores, while ESPB and WI are also alternative analgesic options for these surgeries. However, further studies are needed to determine the optimal method of providing regional analgesia after lumbar spine surgery.
各种区域麻醉技术被用于减轻接受腰椎手术的患者的术后疼痛。传统上,外科医生广泛使用局部麻醉剂进行伤口浸润(WI)。最近,其他区域镇痛技术,如竖脊肌平面阻滞(ESPB)和胸腰椎筋膜平面(TLIP)阻滞,被用于多模式镇痛。作者旨在通过网络荟萃分析来确定这些技术的相对疗效。
作者检索了 PubMed、EMBASE、Cochrane 对照图书馆和 Google Scholar 数据库,以确定比较以下干预措施镇痛效果的所有随机对照试验:ESPB、TLIP 阻滞、WI 技术和对照组。主要终点是术后 24 小时内的阿片类药物消耗,而术后三个不同时间段的疼痛评分是次要目标。
作者纳入了 34 项随机对照试验,共纳入了 2365 名患者的数据。与对照组相比,TLIP 显示出最大程度地减少阿片类药物消耗[平均差异(MD)=-15.0mg;95%可信区间:-18.8 至-11.2]。在疼痛评分方面,TLIP 在所有时间段与对照组相比都有最大的效果(MD=-1.9 在早期,-1.4 在中期,-0.9 在晚期)。ESPB 的注射水平在每项研究中都不同。当仅将 ESPB 的手术部位注射纳入网络荟萃分析时,与 TLIP 相比没有差异(MD=1.0mg;95%可信区间:-3.6 至 5.6)。
TLIP 在腰椎手术后的阿片类药物消耗和疼痛评分方面显示出最大的镇痛效果,而 ESPB 和 WI 也是这些手术的替代镇痛选择。然而,需要进一步的研究来确定腰椎手术后提供区域镇痛的最佳方法。