Division of Reproductive Biology, Maternal and Child Health, Indian Council of Medical Research, New Delhi, India.
Division of Bacteriology, ICMR- Regional Medical Research Centre, NE Region, Dibrugarh, Assam, India.
Indian J Med Res. 2022 Oct-Nov;156(4&5):579-587. doi: 10.4103/ijmr.ijmr_1374_21.
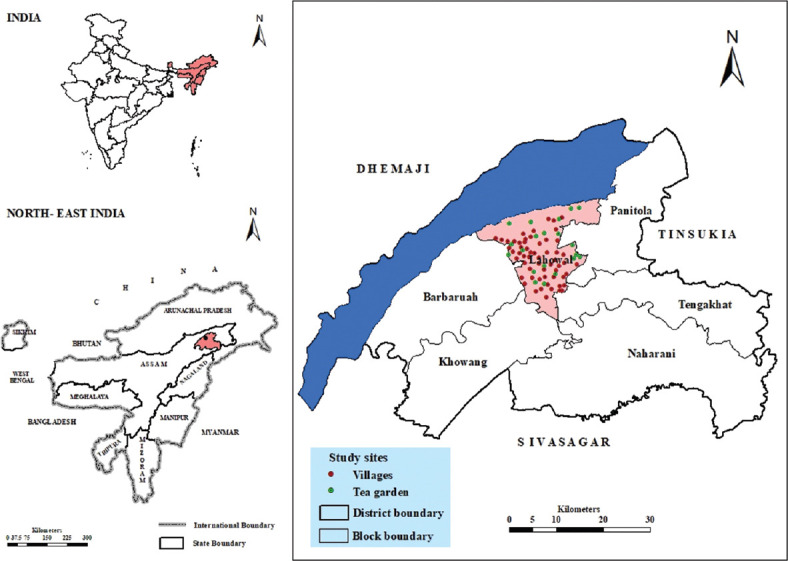
Dibrugarh Health and Demographic Surveillance System (Dibrugarh-HDSS), was started in the year 2019 with the objective to create the health and demographic database of a population from a defined geographical area and a surveillance system for providing technical assistance for the implementation of programmes and formulating intervention strategies for reducing disease morbidities and mortalities in the population. Dibrugarh-HDSS adopted a panel design and covered 60 contiguous villages and 20 tea gardens. Line listing of all the households was conducted and a unique identification number detailing State, district, village/tea garden and serial number was provided along with geotagging. Detailed sociodemographic variables, anthropometric measurements (subjects ≥five years) and blood pressure data (subjects ≥18 yr), disease morbidity and mortality were collected. All data were collected in pre-designed and pre-tested questionnaires using a mobile application package developed for this purpose. Dibrugarh-HDSS included a total of 106,769 individuals (rural: 46,762, tea garden: 60,007) with 52,934 males (49.6%) and 53,835 females (50.4%). The number of females per thousand males were significantly higher (1042 in tea garden vs. 985 in rural populations) in the tea-garden community as compared to the village population. More than one-third (35.1%) of tea populations were illiterate compared to the rural population (17.1%). Villagers had significantly higher body mass index than the tea-garden community. The overall prevalence of hypertension (adjusted for age) was 29.4 vs. 28.2 per cent, respectively, for the village and tea-garden population. For both these communities, males (village=30.8%, tea garden=31.1%) showed a higher prevalence of hypertension (adjusted for age) than females (village=28.2%, tea garden=25.8%). The findings of the present study give an insight into the profile of the native rural and tea-garden populations that will help to identify risk factors of different health problems, review the effectiveness of different ongoing programmes, implement intervention strategies for reducing morbidity and mortality and assist the State health authorities in prioritizing their resource allocation and implementation strategies.
迪布鲁加尔健康与人口监测系统(Dibrugarh-HDSS)于 2019 年启动,旨在创建一个特定地理区域人群的健康和人口数据库,以及一个监测系统,为实施各项方案提供技术援助,并制定减少人群疾病发病率和死亡率的干预策略。Dibrugarh-HDSS 采用面板设计,覆盖 60 个连续村庄和 20 个茶园。对所有家庭进行了清单编制,并提供了一个详细的州、区、村庄/茶园和序列号的唯一识别号码,并进行了地理标记。收集了详细的社会人口学变量、人体测量数据(五岁及以上)和血压数据(十八岁及以上)、疾病发病率和死亡率。所有数据均使用为此目的开发的移动应用程序包,根据预设计和预测试的问卷进行收集。迪布鲁加尔健康与人口监测系统共包括 106769 人(农村:46762 人,茶园:60007 人),其中男性 52934 人(49.6%),女性 53835 人(50.4%)。茶园社区每千名男性中的女性人数明显高于农村人口(茶园为 1042 人,农村为 985 人)。与农村人口相比(17.1%),超过三分之一(35.1%)的茶园人口是文盲。与茶园社区相比,村民的身体质量指数明显更高。调整年龄后的高血压总体患病率分别为农村人口的 29.4%和茶园人口的 28.2%。对于这两个社区,男性(农村=30.8%,茶园=31.1%)的高血压(调整年龄后)患病率均高于女性(农村=28.2%,茶园=25.8%)。本研究的结果提供了对当地农村和茶园人口特征的深入了解,有助于确定不同健康问题的风险因素,审查不同现有方案的有效性,实施减少发病率和死亡率的干预策略,并协助邦卫生当局确定资源分配和实施策略的优先顺序。