Institute for Healthcare Policy and Innovation, University of Michigan Medical School, Ann Arbor.
Department of Surgery, University of Michigan Medical School, Ann Arbor.
JAMA Netw Open. 2023 Mar 1;6(3):e232109. doi: 10.1001/jamanetworkopen.2023.2109.
There has been a paucity of research examining the risk and cost of readmission among patients with Alzheimer disease and related dementias (ADRD) after a planned hospitalization for a broad set of medical and surgical procedures.
To examine 30-day readmission rates and episode costs, including readmission costs, for patients with ADRD compared with their counterparts without ADRD across Michigan hospitals.
DESIGN, SETTING, AND PARTICIPANTS: This retrospective cohort study used 2012 to 2017 Michigan Value Collaborative data across different medical and surgical services stratified by ADRD diagnosis. A total of 66 676 admission episodes of care that occurred between January 1, 2012, and June 31, 2017, were identified for patients with ADRD using International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) and International Statistical Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10-CM) diagnostic codes for ADRD, along with 656 235 admission episodes in patients without ADRD. Using a generalized linear model framework, this study risk adjusted, price standardized, and performed episode payment winsorization. Payments were risk adjusted for age, sex, Hierarchical Condition Categories, insurance type, and prior 6-month payments. Selection bias was accounted for using multivariable logistic regression with propensity score matching without replacement using calipers. Data analysis was performed from January to December 2019.
Presence of ADRD.
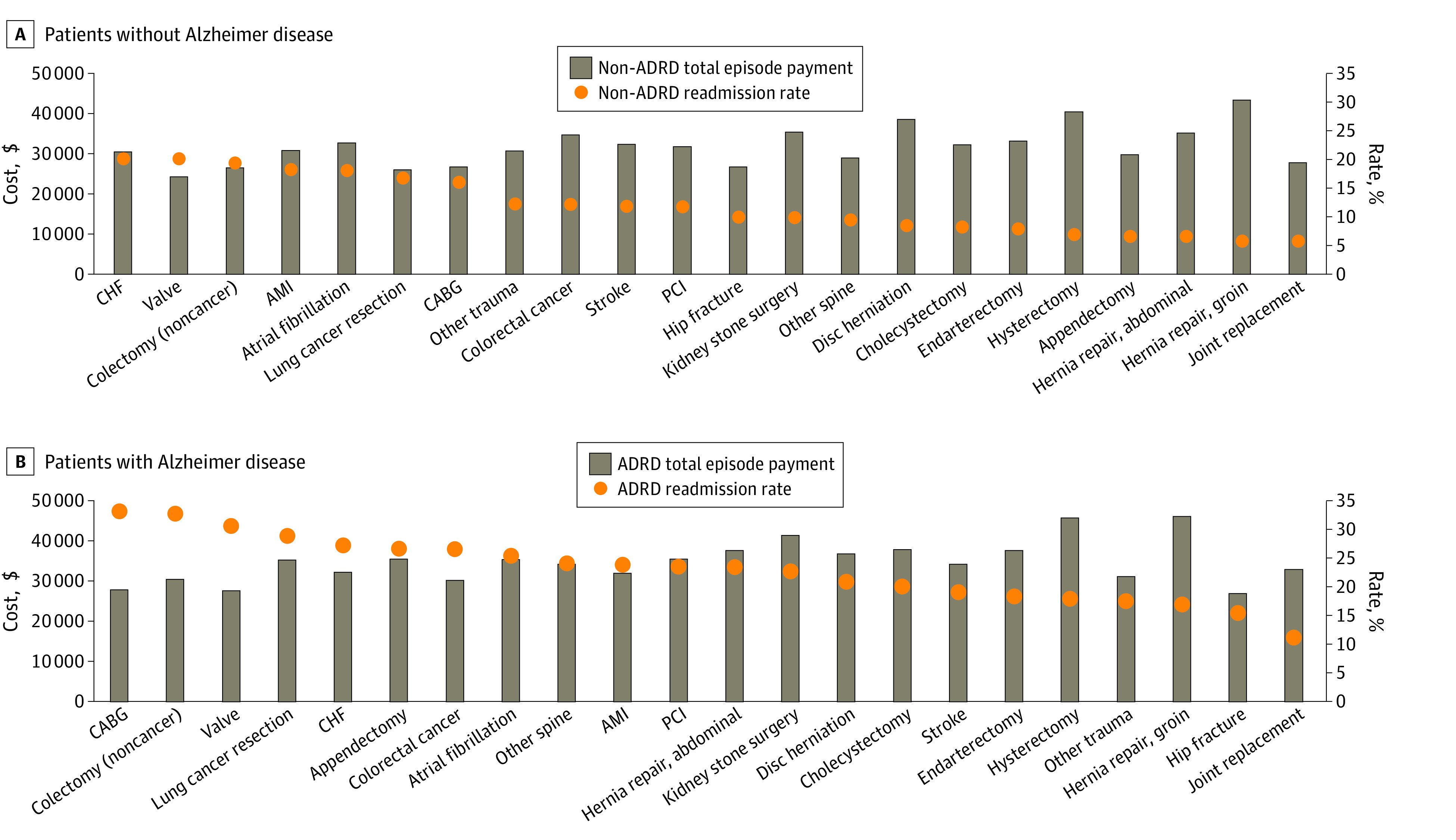
Main outcomes were 30-day readmission rate at the patient and county levels, 30-day readmission cost, and 30-day total episode cost across 28 medical and surgical services.
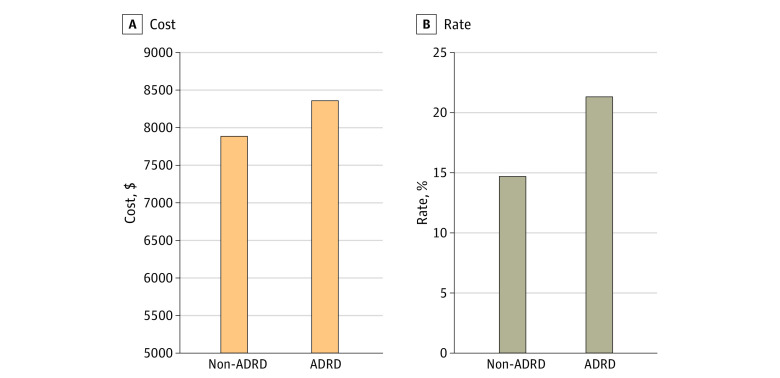
The study included 722 911 hospitalization episodes, of which 66 676 were related to patients with ADRD (mean [SD] age, 83.4 [8.6] years; 42 439 [63.6%] female) and 656 235 were related to patients without ADRD (mean [SD] age, 66.0 [15.4] years; 351 246 [53.5%] female). After propensity score matching, 58 629 hospitalization episodes were included for each group. Readmission rates were 21.5% (95% CI, 21.2%-21.8%) for patients with ADRD and 14.7% (95% CI, 14.4%-15.0%) for patients without ADRD (difference, 6.75 percentage points; 95% CI, 6.31-7.19 percentage points). Cost of 30-day readmission was $467 higher (95% CI of difference, $289-$645) among patients with ADRD ($8378; 95% CI, $8263-$8494) than those without ($7912; 95% CI, $7776-$8047). Across all 28 service lines examined, total 30-day episode costs were $2794 higher for patients with ADRD vs patients without ADRD ($22 371 vs $19 578; 95% CI of difference, $2668-$2919).
In this cohort study, patients with ADRD had higher readmission rates and overall readmission and episode costs than their counterparts without ADRD. Hospitals may need to be better equipped to care for patients with ADRD, especially in the postdischarge period. Considering that any type of hospitalization may put patients with ADRD at a high risk of 30-day readmission, judicious preoperative assessment, postoperative discharge, and care planning are strongly advised for this vulnerable patient population.
在计划住院接受广泛的医疗和手术治疗后,针对阿尔茨海默病和相关痴呆症 (ADRD) 患者的再入院风险和成本,研究相对较少。
检查密歇根州医院的 ADRD 患者与无 ADRD 患者相比的 30 天再入院率和住院费用,包括再入院费用。
设计、地点和参与者:这是一项回顾性队列研究,使用密歇根价值合作组织 2012 年至 2017 年不同医疗和手术服务的数据,按 ADRD 诊断分层。通过使用国际疾病分类,第九修订版,临床修正 (ICD-9-CM) 和国际疾病分类,第十版,临床修正 (ICD-10-CM) 诊断代码,共确定了 66676 例 ADRD 患者的入院治疗发作,以及 656235 例无 ADRD 患者的入院治疗发作。使用广义线性模型框架,本研究对风险进行了调整、价格进行了标准化,并进行了住院费用 winsorization。付款按年龄、性别、分层条件类别、保险类型和前 6 个月的付款进行风险调整。使用多变量逻辑回归和无替换的倾向评分匹配(使用卡尺)来考虑选择偏差。数据分析于 2019 年 1 月至 12 月进行。
ADRD 的存在。
主要结果是患者和县级 30 天再入院率、30 天再入院费用和 28 种医疗和手术服务的 30 天总住院费用。
本研究包括 722911 例住院发作,其中 66676 例与 ADRD 患者有关(平均[SD]年龄,83.4[8.6]岁;42439[63.6%]女性),656235 例与无 ADRD 患者有关(平均[SD]年龄,66.0[15.4]岁;351246[53.5%]女性)。在进行倾向评分匹配后,每组纳入 58629 例住院发作。ADRD 患者的再入院率为 21.5%(95%CI,21.2%-21.8%),无 ADRD 患者的再入院率为 14.7%(95%CI,14.4%-15.0%)(差异为 6.75 个百分点;95%CI,6.31-7.19 个百分点)。ADRD 患者 30 天再入院费用为 8378 美元(95%CI 为 8263-8494 美元),高于无 ADRD 患者的 7912 美元(95%CI 为 7776-8047 美元)(差异为 467 美元;95%CI,289-645 美元)。在所有检查的 28 种服务线中,ADRD 患者的 30 天总住院费用比无 ADRD 患者高 2794 美元(22371 美元比 19578 美元;95%CI 差异为 2668-2919 美元)。
在这项队列研究中,ADRD 患者的再入院率和总体再入院和住院费用均高于无 ADRD 患者。医院可能需要更好地为 ADRD 患者提供护理,尤其是在出院后期间。考虑到任何类型的住院治疗都可能使 ADRD 患者面临 30 天再入院的高风险,强烈建议为这一脆弱患者群体进行术前评估、术后出院和护理计划。