Department of Obstetrics and Gynaecology, University Medical Center Utrecht, Utrecht, Netherlands.
Department of Obstetrics and Gynaecology, Amsterdam University Medical Center, location AMC, Amsterdam, Netherlands.
BMJ Open. 2023 Mar 17;13(3):e070729. doi: 10.1136/bmjopen-2022-070729.
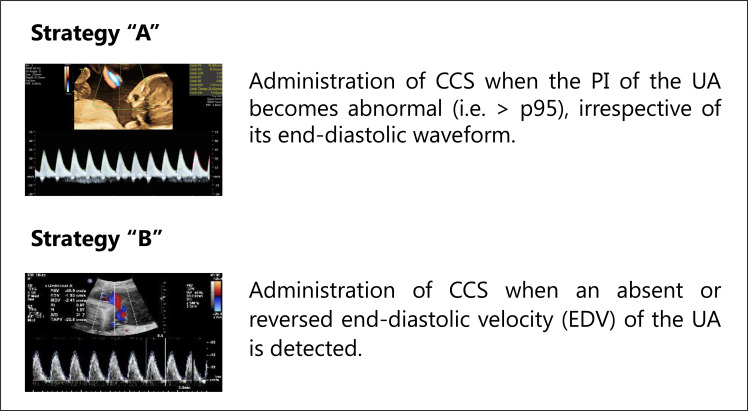
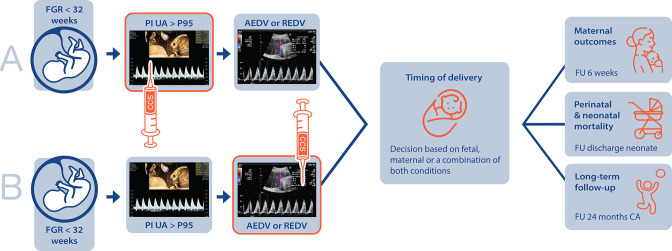
Early-onset fetal growth restriction (FGR) requires timely, often preterm, delivery to prevent fetal hypoxia causing stillbirth or neurologic impairment. Antenatal corticosteroids (CCS) administration reduces neonatal morbidity and mortality following preterm birth, most effectively when administered within 1 week preceding delivery. Optimal timing of CCS administration is challenging in early-onset FGR, as the exact onset and course of fetal hypoxia are unpredictable. International guidelines do not provide a directive on this topic. In the Netherlands, two timing strategies are commonly practiced: administration of CCS when the umbilical artery shows (A) a pulsatility index above the 95th centile and (B) absent or reversed end-diastolic velocity (a more progressed disease state). This study aims to (1) use practice variation to compare CCS timing strategies in early-onset FGR on fetal and neonatal outcomes and (2) develop a dynamic tool to predict the time interval in days until delivery, as a novel timing strategy for antenatal CCS in early-onset FGR.
A multicentre, retrospective cohort study will be performed including pregnancies complicated by early-onset FGR in six tertiary hospitals in the Netherlands in the period between 2012 and 2021 (estimated sample size n=1800). Main exclusion criteria are multiple pregnancies and fetal congenital or genetic abnormalities. Routinely collected data will be extracted from medical charts. Primary outcome for the comparison of the two CCS timing strategies is a composite of perinatal, neonatal and in-hospital mortality. Secondary outcomes include the COSGROVE core outcome set for FGR. A multivariable, mixed-effects model will be used to compare timing strategies on study outcomes. Primary outcome for the dynamic prediction tool is 'days until birth'.
The need for ethical approval was waived by the Ethics Committee (University Medical Center Utrecht). Results will be published in open-access, peer-reviewed journals and disseminated by presentations at scientific conferences.
ClinicalTrials.gov: NCT05606497.
早期胎儿生长受限(FGR)需要及时分娩,通常是早产,以防止胎儿缺氧导致死产或神经损伤。产前皮质类固醇(CCS)的应用可降低早产儿的发病率和死亡率,在分娩前 1 周内应用效果最佳。早期胎儿生长受限时,CCS 的最佳应用时机具有挑战性,因为胎儿缺氧的确切发作和过程是不可预测的。国际指南对此没有给出指导意见。在荷兰,两种时间策略通常被采用:当脐动脉搏动指数高于第 95 百分位数时(A),或当脐动脉无舒张末期血流或出现反向血流时(B)(疾病状态更为严重),给予 CCS。本研究旨在(1)利用实践差异比较早期胎儿生长受限中两种 CCS 时间策略对胎儿和新生儿结局的影响,(2)开发一种新的时间策略,用于预测直至分娩的天数间隔,作为早期胎儿生长受限中产前 CCS 的新时间策略。
一项多中心、回顾性队列研究将在荷兰六家三级医院进行,纳入 2012 年至 2021 年期间患有早期胎儿生长受限的妊娠(估计样本量 n=1800)。主要排除标准是多胎妊娠和胎儿先天性或遗传性异常。将从病历中提取常规收集的数据。两种 CCS 时间策略比较的主要结局是围产儿、新生儿和院内死亡率的复合结局。次要结局包括胎儿生长受限的 COSGROVE 核心结局集。将使用多变量混合效应模型比较两种时间策略对研究结局的影响。动态预测工具的主要结局是“分娩前的天数”。
乌得勒支大学医学中心伦理委员会豁免了伦理批准的需要。结果将发表在开放获取、同行评议的期刊上,并通过在科学会议上的演讲进行传播。
ClinicalTrials.gov:NCT05606497。