Department of Internal Medicine, National Taiwan University Hospital, Taipei, Taiwan; Graduate Institute of Clinical Medicine, National Taiwan University College of Medicine, Taipei, Taiwan.
Department of Internal Medicine, National Taiwan University Hospital, Taipei, Taiwan; National Institutes of Infectious Diseases and Vaccinology, National Health Research Institutes, Miaoli, Taiwan.
J Formos Med Assoc. 2023 Aug;122(8):766-775. doi: 10.1016/j.jfma.2023.02.008. Epub 2023 Mar 8.
COVID-19 rebound is usually reported among patients experiencing concurrent symptomatic and viral rebound. But longitudinal viral RT-PCR results from early stage to rebound of COVID-19 was less characterized. Further, identifying the factors associated with viral rebound after nirmatrelvir-ritonavir (NMV/r) and molnupiravir may expand understanding of COVID-19 rebound.
We retrospectively analyzed clinical data and sequential viral RT-PCR results from COVID-19 patients receiving oral antivirals between April and May, 2022. Viral rebound was defined by the degree of viral load increase (ΔCt ≥ 5 units).
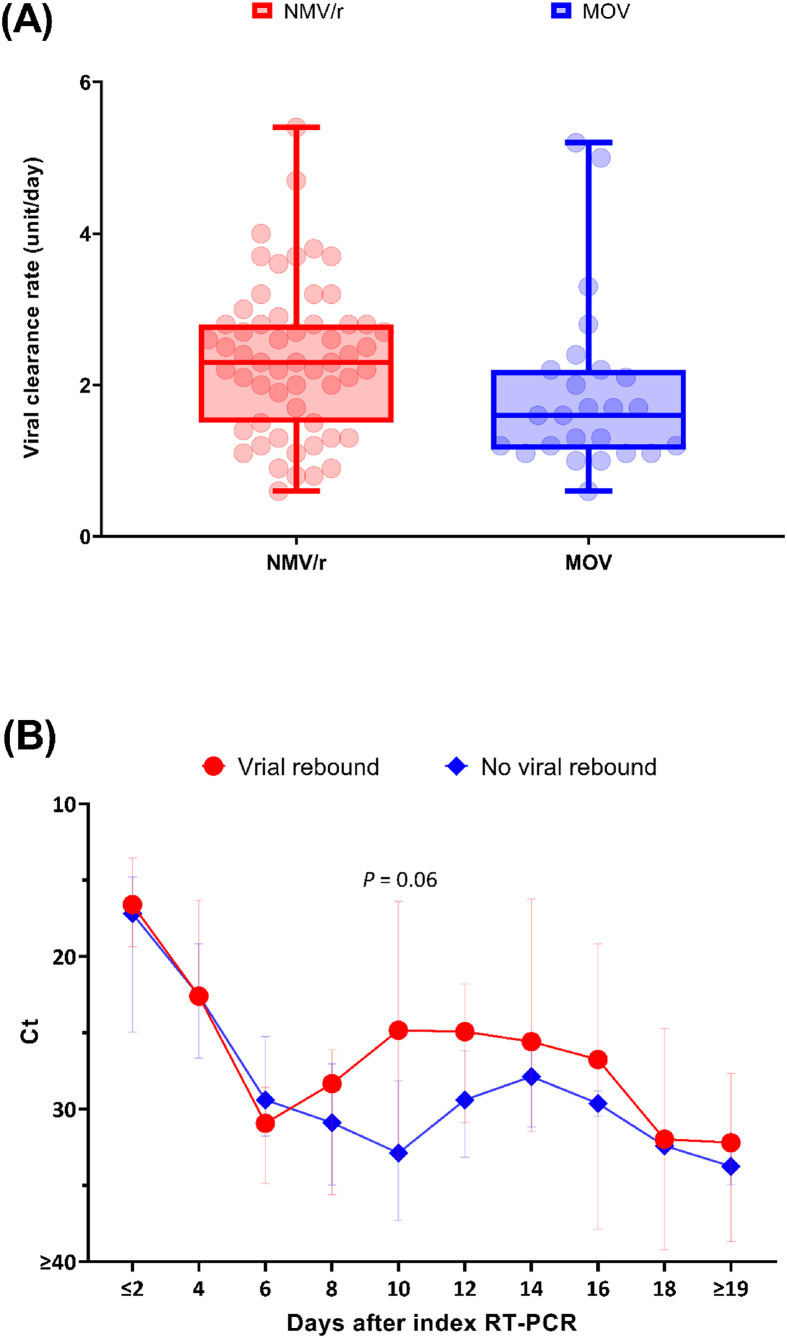
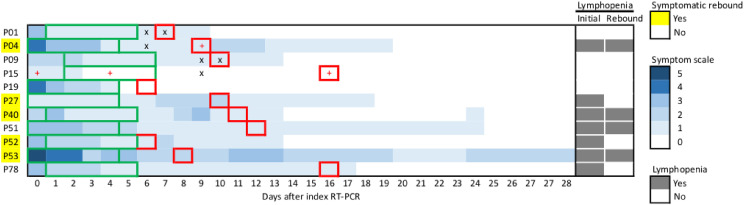
A total of 58 and 27 COVID-19 patients taking NMV/r and molnupiravir, respectively, were enrolled. Patients receiving NMV/r were younger, had fewer risk factors for disease progression and faster viral clearance rate compared to those receiving molnupiravr (All P < 0.05). The overall proportion of viral rebound (n = 11) was 12.9%, which was more common among patients receiving NMV/r (10 [17.2%] vs. 1 [3.7%], P = 0.16). Of them, 5 patients experienced symptomatic rebound, suggesting the proportion of COVID-19 rebound was 5.9%. The median interval to viral rebound was 5.0 (interquartile range, 2.0-8.0) days after completion of antivirals. Initial lymphopenia (<0.8 × 10/L) was associated with viral rebound among overall population (adjusted odds ratio [aOR], 5.34; 95% confidence interval [CI], 1.33-21.71), and remained significant (aOR, 4.50; 95% CI, 1.05-19.25) even when patients receiving NMV/r were considered.
Our data suggest viral rebound after oral antivirals may be more commonly observed among lymphopenic individuals in the context of SARS-CoV-2 Omicron BA.2 variant.
COVID-19 反弹通常在同时出现症状和病毒反弹的患者中报告。但 COVID-19 早期到反弹阶段的纵向病毒 RT-PCR 结果特征描述较少。此外,确定 nirmatrelvir-ritonavir(NMV/r)和 molnupiravir 治疗后与病毒反弹相关的因素可能会增加对 COVID-19 反弹的理解。
我们回顾性分析了 2022 年 4 月至 5 月期间接受口服抗病毒药物治疗的 COVID-19 患者的临床数据和连续病毒 RT-PCR 结果。病毒反弹定义为病毒载量增加程度(ΔCt≥5 单位)。
共纳入 58 例接受 NMV/r 和 27 例接受 molnupiravir 的 COVID-19 患者。与接受 molnupiravr 的患者相比,接受 NMV/r 的患者年龄更小,疾病进展的危险因素更少,病毒清除率更快(均 P<0.05)。病毒反弹(n=11)的总比例为 12.9%,在接受 NMV/r 的患者中更为常见(10 [17.2%] 例 vs. 1 [3.7%],P=0.16)。其中 5 例患者出现症状性反弹,提示 COVID-19 反弹的比例为 5.9%。抗病毒治疗完成后,病毒反弹的中位时间为 5.0(四分位距,2.0-8.0)天。全人群中初始淋巴细胞减少症(<0.8×10/L)与病毒反弹相关(调整后比值比[aOR],5.34;95%置信区间[CI],1.33-21.71),即使考虑到接受 NMV/r 的患者,该结果仍具有统计学意义(aOR,4.50;95%CI,1.05-19.25)。
我们的数据表明,在 SARS-CoV-2 Omicron BA.2 变异株背景下,口服抗病毒药物后病毒反弹在淋巴细胞减少症个体中可能更为常见。