South Africa Medical Research Council Vaccines and Infectious Diseases Analytics Research Unit, University of the Witwatersrand, Johannesburg, South Africa.
South Africa Medical Research Council Vaccines and Infectious Diseases Analytics Research Unit, University of the Witwatersrand, Johannesburg, South Africa; Department of Pediatrics, Amsterdam University Medical Center, Amsterdam, Netherlands.
Lancet Child Adolesc Health. 2023 May;7(5):326-335. doi: 10.1016/S2352-4642(23)00025-1. Epub 2023 Mar 16.
Pneumococcal conjugate vaccine (PCV) immunisation has reduced vaccine-serotype colonisation and invasive pneumococcal disease in South Africa, providing the opportunity to consider transitioning from a two-dose (2 + 1) to one-dose (1 + 1) primary series and a booster dose.
In this single-centre, open-label, randomised trial done in South Africa, infants aged 35-49 days without HIV infection, without childhood immunisations except for BCG and polio, and with gestation age at delivery of at least 37 weeks of age, a birthweight of at least 2500 g, and weight of at least 3500 g at the time of enrolment were randomly assigned (1:1:1:1:1:1), through block randomisation (block size of 30), to receive a single priming dose of ten-valent PCV (PCV10) or 13-valent PCV (PCV13) at either 6 weeks (6-week 1 + 1 group) or 14 weeks (14-week 1 + 1 group), compared with two priming doses at 6 weeks and 14 weeks (2 + 1 group), followed by a booster dose at 9 months of age in all groups. The primary objective of the trial has been published previously. We report the secondary objective of the effect of alternative doses of PCV10 and PCV13 on serotype-specific Streptococcus pneumoniae colonisation at 9 months, 15 months, and 18 months of age and a further exploratory analysis in which we assessed non-inferiority of serotype-specific serum IgG geometric mean concentrations 1 month after the booster (10 months of age) and the percentage of participants with serotype-specific IgG titre above the putative thresholds associated with a risk reduction of serotype-specific colonisation between the 1 + 1 and 2 + 1 groups for both vaccines. Non-inferiority was established if the lower limit of the 95% CI for the difference between the proportion of participants (1 + 1 group vs 2 + 1 group) above the putative thresholds was greater than or equal to -10%. All analyses were done in the modified intention-to-treat population, which included all participants who received PCV10 or PCV13 according to assigned randomisation group and for whom laboratory results were available. The trial is registered with ClinicalTrials.gov, NCT02943902.
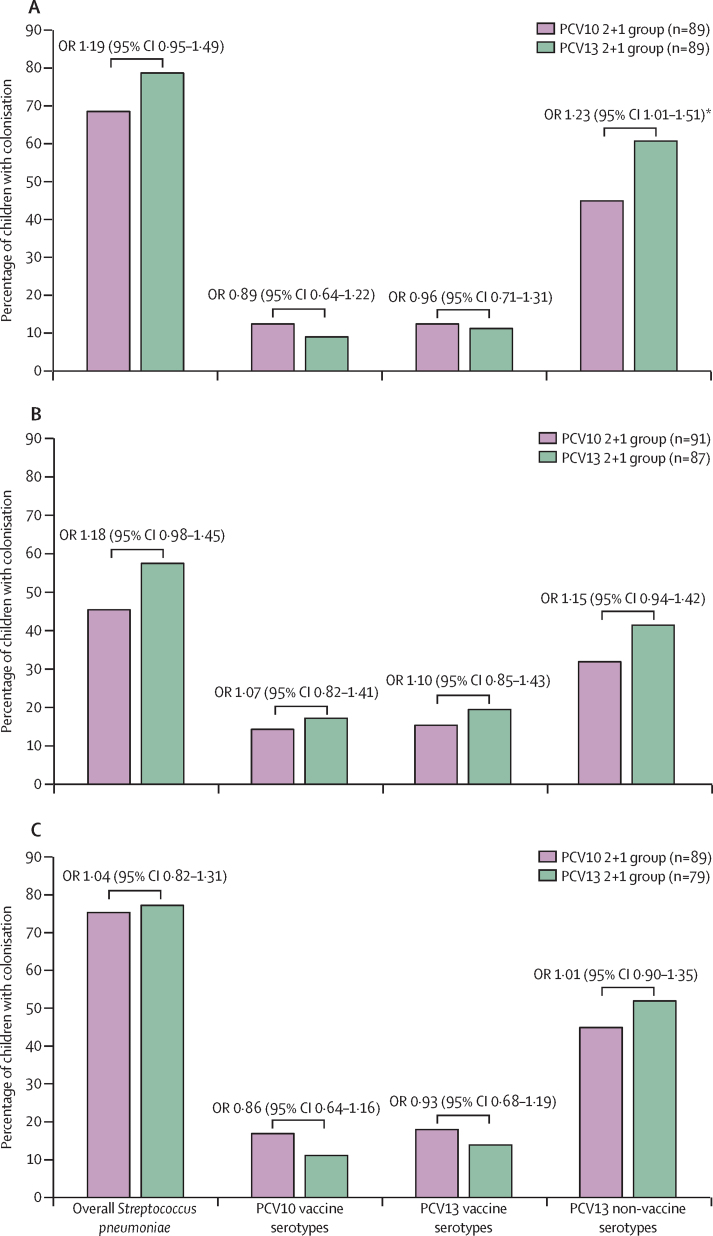
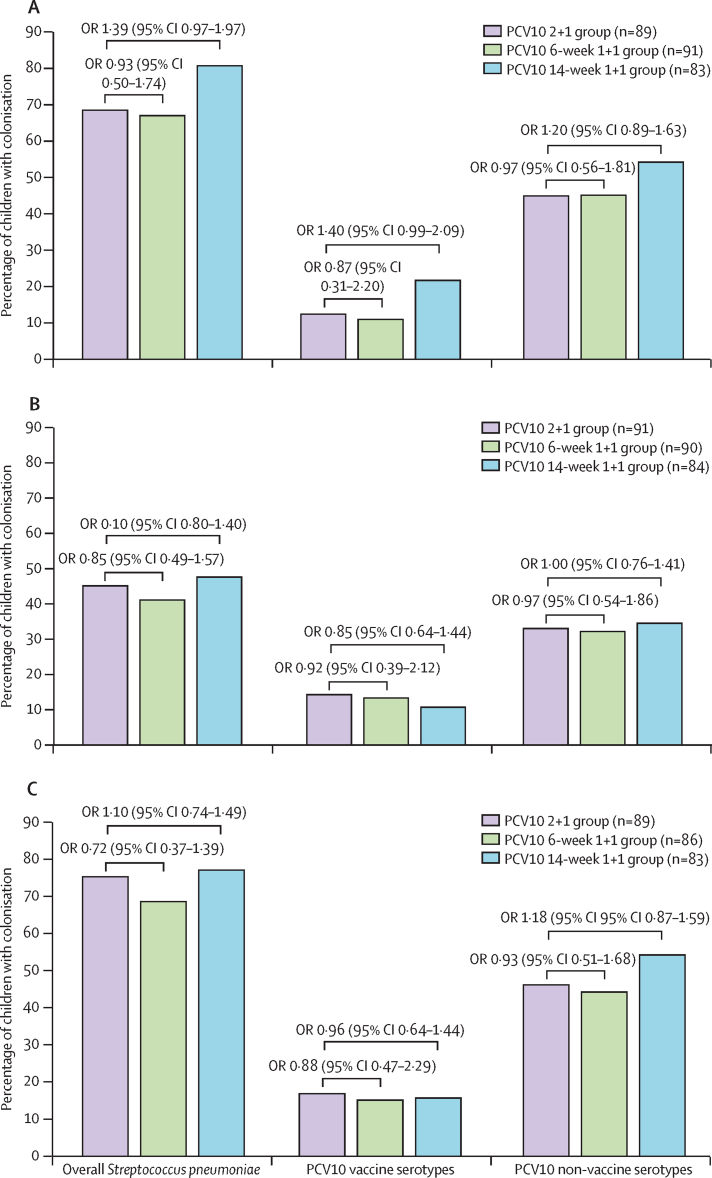
1564 nasopharyngeal swabs were available for molecular serotyping from 600 infants who were enrolled (100 were randomly assigned to each of the six study groups) between Jan 9 and Sept 20, 2017. There was no significant difference in the prevalence of overall or non-vaccine serotype colonisation between all PCV13 or PCV10 groups. PCV13 serotype colonisation was lower at 15 months of age in the 14-week 1 + 1 group than in the 2 + 1 group (seven [8%] of 85 vs 17 [20%] of 87; odds ratio 0·61 [95% CI 0·38-0·97], p=0·037), but no difference was seen at 9 months (nine [11%] of 86 vs ten [11%] of 89; 0·92 [0·60-1·55], p=0·87) or 18 months (nine [11%] of 85 vs 11 [14%] of 87; 0·78 [0·45-1·22], p=0·61). Compared with the PCV13 2 + 1 group, both PCV13 1 + 1 groups did not meet the non-inferiority criteria for serotype-specific anti-capsular antibody concentrations above the putative thresholds purportedly associated with risk reduction for colonisation; however, the PCV10 14-week 1 + 1 group was non-inferior to the PCV10 2 + 1 group.
The serotype-specific colonisation data reported in this study together with the primary immunogenicity endpoints of the control trial support transitioning to a reduced 1 + 1 schedule in South Africa. Ongoing monitoring of colonisation should, however, be undertaken immediately before and after transitioning to a PCV 1 + 1 schedule to serve as an early indicator of whether PCV 1 + 1 could lead to an increase in vaccine-serotype disease.
The Bill & Melinda Gates Foundation.
肺炎球菌结合疫苗(PCV)免疫接种减少了南非疫苗血清型定植和侵袭性肺炎球菌病,为从两剂(2+1)过渡到一剂(1+1)基础系列和加强剂量提供了机会。
在南非进行的这项单中心、开放性、随机试验中,纳入了无 HIV 感染、除卡介苗和脊髓灰质炎疫苗外无儿童期免疫接种、分娩时胎龄至少 37 周、出生体重至少 2500g、入组时体重至少 3500g 的 35-49 日龄婴儿。通过区组随机化(区组大小为 30),将婴儿按照 1:1:1:1:1:1 的比例随机分配,接受 10 价 PCV(PCV10)或 13 价 PCV(PCV13)的单剂初免,接种时间分别为 6 周(6 周 1+1 组)或 14 周(14 周 1+1 组),与 6 周和 14 周接种两剂(2+1 组)相比,所有组别的加强剂量均在 9 个月龄时接种。该试验的主要目标已经公布。我们报告了替代剂量的 PCV10 和 PCV13 对 9 个月、15 个月和 18 个月时血清型特异型肺炎链球菌定植的影响,以及一项进一步的探索性分析,评估了在加强剂量后 1 个月(10 个月龄)时血清 IgG 几何平均浓度的非劣效性,以及与两剂 1+1 组相比,两种疫苗的血清型特异 IgG 滴度高于假定阈值与血清型特异定植风险降低相关的参与者比例。如果差异的 95%置信区间下限大于或等于-10%,则认为非劣效性成立。所有分析均在改良意向治疗人群中进行,该人群包括根据随机分组接受 PCV10 或 PCV13 且可获得实验室结果的所有参与者。该试验在 ClinicalTrials.gov 上注册,编号为 NCT02943902。
2017 年 1 月 9 日至 9 月 20 日,纳入了 600 名婴儿,共采集了 1564 份鼻咽拭子进行分子血清型分析,其中 100 名婴儿随机分配到六个研究组中的每个组。所有 PCV13 或 PCV10 组之间的总定植率或非疫苗血清型定植率无显著差异。14 周 1+1 组中 PCV13 血清型定植率在 15 个月龄时低于 2+1 组(85 名婴儿中 7 名[8%]vs.87 名婴儿中 17 名[20%];比值比 0.61[95%置信区间 0.38-0.97],p=0.037),但在 9 个月龄(86 名婴儿中 9 名[11%]vs.89 名婴儿中 10 名[11%];0.92[0.60-1.55],p=0.87)或 18 个月龄(85 名婴儿中 9 名[11%]vs.87 名婴儿中 11 名[14%];0.78[0.45-1.22],p=0.61)时无差异。与 PCV13 2+1 组相比,两组 PCV13 1+1 组均未达到血清型特异抗荚膜抗体浓度高于假定阈值的非劣效性标准,这些阈值据称与降低定植风险相关;然而,PCV10 14 周 1+1 组与 PCV10 2+1 组相当。
本研究报告的血清型定植数据,加上对照试验的主要免疫原性终点结果,支持在南非过渡到减少的 1+1 方案。在过渡到 PCV 1+1 方案之前和之后,应立即进行定植监测,作为疫苗血清型疾病增加的早期指标。
比尔及梅琳达·盖茨基金会。