Sunderkötter Cord, Golle Linda, Pillebout Evangéline, Michl Christiane
Department of Dermatology and Venereology, University Hospital Halle, Martin-Luther-University Halle-Wittenberg, Halle, Germany.
Laboratory Nephrology Unit, Saint Louis Hospital, INSERM 1149, CRI, Paris, France.
Front Med (Lausanne). 2023 Mar 3;10:1103065. doi: 10.3389/fmed.2023.1103065. eCollection 2023.
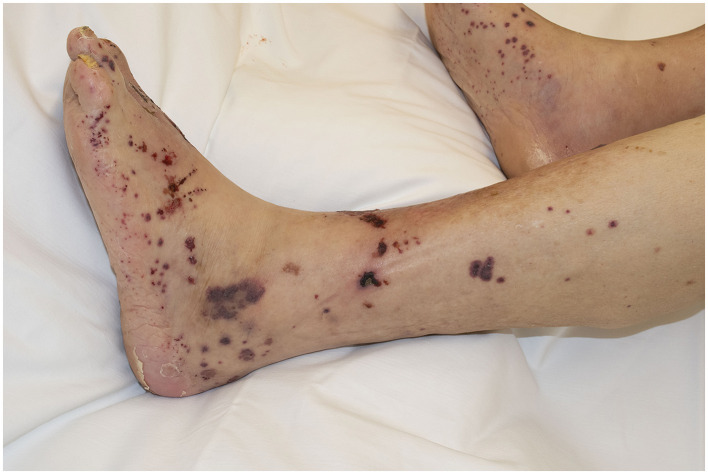
Immune complex (IC) vasculitides present inflammations of vessel walls associated with perivascular deposition of immunoglobulins (Igs), mostly ICs. They encompass systemic and skin-limited variants of IgA vasculitis (IgAV), cryoglobulinemic vasculitis (CV), rheumatoid, lupus, and hypocomplementemic vasculitides, serum sickness cutaneous IgM/IgG (non-IgA) vasculitis, and recurrent macular (hypergammaglobulinemic or exertion-induced) vasculitis. Serum sickness and CV fulfill the criteria of a type III hypersensitivity immune reaction as large lattices of the IC precipitate at vessel walls and activate polymorphonuclear neutrophils (PMNs). Immunoglobulin-A vasculitis differs with regard to the causes of perivascular deposition of ICs since here many IgA1 molecules are hypoglycosylated (Gd-IgA1), which appears to facilitate their perivascular deposition in skin and mesangium (via e.g. CD71). The reasons for increased generation of immunoglobulins or formation of IC and their perivascular deposition in either skin or systemic organs are different and not fully explored. A common denominator of OC vasculitides is the activation of PMNs near the vessel wall Fcy or Fcα receptors. Acute episodes of IgAV additionally require PMNs to become preactivated by IgA1 or by IC already in circulation. This intravascular priming results in increased adherence and subsequently vessel-destructive NETosis when they encounter IgA deposited at the vessel walls. Binding of IgA1 to PMNs in blood stream is associated with increased serum levels of hypogalactosidated IgA1. The characteristic clinical picture of IgAV (and also of so-called IgG/IgM vasculitis) comprises palpable or retiform purpura with a clear predilection for lower legs, probably due to stasis-related reduction in blood velocity, while in other IC vasculitides, additional factors influence the sites of vasculitides. Our knowledge of distinct forms and different pathophysiological pathways of IC vasculitides may lead to in efficacious or targeted therapies. Antibodies to complement components or intestinal budesonide for IgAV are promising agents (the latter suppresses the pathophysiologically related IgA nephropathy by reducing the generation of mucosal IgA.
免疫复合物(IC)性血管炎表现为血管壁炎症,伴有免疫球蛋白(Igs),主要是IC在血管周围沉积。它们包括IgA血管炎(IgAV)、冷球蛋白血症性血管炎(CV)、类风湿性、狼疮性和低补体血症性血管炎、血清病性皮肤IgM/IgG(非IgA)血管炎以及复发性黄斑(高球蛋白血症性或运动诱发)血管炎的系统性和皮肤局限性变体。血清病和CV符合III型超敏免疫反应的标准,因为IC的大晶格在血管壁沉淀并激活多形核中性粒细胞(PMN)。IgA血管炎在IC血管周围沉积的原因方面有所不同,因为这里许多IgA1分子低糖基化(Gd-IgA1),这似乎促进了它们在皮肤和系膜中的血管周围沉积(例如通过CD71)。免疫球蛋白生成增加或IC形成及其在皮肤或全身器官中血管周围沉积的原因各不相同,尚未完全阐明。IC血管炎的一个共同特征是血管壁附近的PMN通过Fcy或Fcα受体激活。IgAV的急性发作还需要PMN被循环中的IgA1或IC预先激活。这种血管内启动导致当它们遇到沉积在血管壁的IgA时,粘附增加并随后发生破坏血管的中性粒细胞胞外陷阱形成。血流中IgA1与PMN的结合与低半乳糖基化IgA1的血清水平升高有关。IgAV(以及所谓的IgG/IgM血管炎)的特征性临床表现包括可触及的或网状紫癜,明显好发于小腿,这可能是由于与淤血相关的血流速度降低,而在其他IC血管炎中,其他因素影响血管炎的部位。我们对IC血管炎不同形式和不同病理生理途径的了解可能会带来有效的或有针对性的治疗。针对补体成分的抗体或用于IgAV的肠道布地奈德是有前景的药物(后者通过减少粘膜IgA的产生来抑制病理生理相关的IgA肾病)。