Jiao Jinghua, Yu Jie, Chen Chenghao, Chen Tian, Zheng Tiehua, He Lejian, Zeng Qi
Department of Thoracic Surgery, Beijing Children's Hospital, Capital Medical University, National Center for Children's Health, Beijing, China.
Department of Anesthesiology, Beijing Children's Hospital, Capital Medical University, National Center for Children's Health, Beijing, China.
Front Pediatr. 2023 Mar 1;11:1144384. doi: 10.3389/fped.2023.1144384. eCollection 2023.
Massive thymic hyperplasia (MTH) is a very rare entity, with fewer than 20 cases reported in the literature in infancy. Most patients have respiratory symptoms and the enlarged thymus gland occupies one side of the thoracic cavity. Posterolateral thoracotomy or median sternotomy is the main treatment for MTH in infants. We report a case of an infant with MTH in which the enlarged thymus occupied his bilateral thoracic cavity and he underwent video-assisted thoracoscopic surgery (VATS). In addition, we reviewed and summarized the relevant literature.
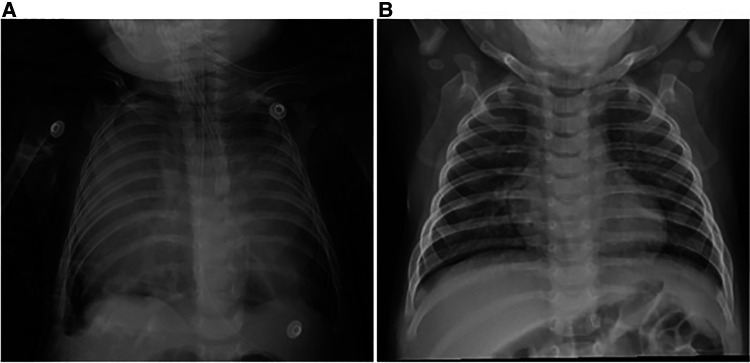
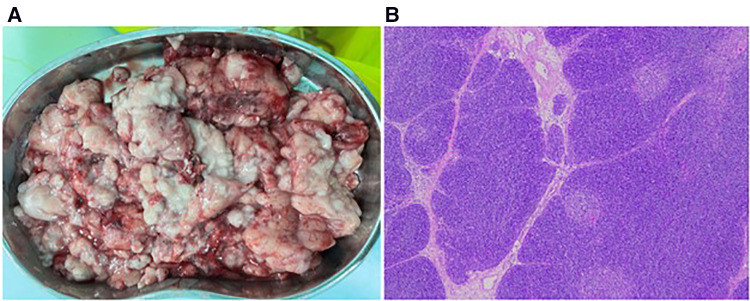
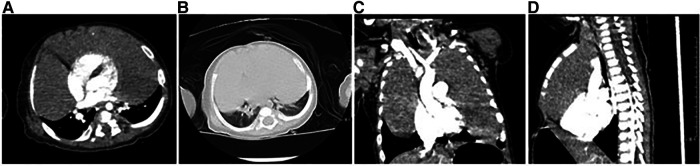
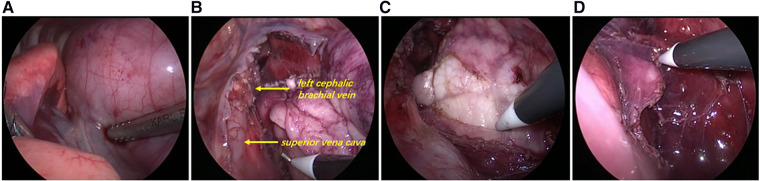
A 4-month-old boy was admitted to the hospital with no apparent cause of dyspnea for 18 days, with cough and sputum. On examination, the patient was found to have cyanotic lips, diminished breath sounds in both lungs, and a positive three concave sign. There was no fever or ptosis. Preoperative imaging showed large soft tissue shadows in the bilateral thoracic cavity, with basic symmetry between the right and left sides. Tumor markers were within the normal range. Ultrasound-guided fine needle biopsy showed normal thymic structures with no evidence of malignancy. As his symptoms worsened, he eventually underwent unilateral thoracic approach video-assisted thoracoscopic exploratory surgery, during which a large mass occupying the bilateral thoracic cavity was removed in a separate block and part of the thymus in the left lobe was preserved. Pathological examination confirmed true thymic hyperplasia (TTH). No relevant complications occurred at the 2-month postoperative follow-up.
In infants, MTH occupying the bilateral thoracic cavity can produce severe respiratory and circulatory symptoms due to occupying effects. Although a definitive preoperative diagnosis is sometimes difficult, after combining computed tomography (CT) and fine needle biopsy to exclude evidence of other malignancies, the enlarged thymus occupying the bilateral thoracic cavity can be resected VATS. Whether the enlarged thymus occupies the bilateral thoracic cavity and the size of the thymus are not absolute contraindications to thoracoscopic surgery. The method is safe, feasible, and minimally invasive to the patient.
巨大胸腺增生(MTH)是一种非常罕见的病症,文献报道婴儿期病例少于20例。大多数患者有呼吸道症状,肿大的胸腺占据胸腔一侧。后外侧开胸术或正中胸骨切开术是婴儿MTH的主要治疗方法。我们报告一例婴儿MTH病例,其肿大的胸腺占据双侧胸腔,接受了电视辅助胸腔镜手术(VATS)。此外,我们回顾并总结了相关文献。
一名4个月大男孩因无明显诱因出现呼吸困难18天,伴有咳嗽、咳痰入院。检查发现患者嘴唇发绀,双肺呼吸音减弱,三凹征阳性。无发热及上睑下垂。术前影像学检查显示双侧胸腔有巨大软组织阴影,左右基本对称。肿瘤标志物在正常范围内。超声引导下细针穿刺活检显示胸腺结构正常,无恶性证据。随着症状加重,他最终接受了单侧胸腔入路电视辅助胸腔镜探查手术,术中将占据双侧胸腔的巨大肿物完整切除,并保留了左叶部分胸腺。病理检查证实为真性胸腺增生(TTH)。术后2个月随访未发生相关并发症。
在婴儿中,占据双侧胸腔的MTH可因占位效应产生严重的呼吸和循环症状。尽管有时术前明确诊断困难,但在结合计算机断层扫描(CT)和细针活检排除其他恶性证据后,可通过VATS切除占据双侧胸腔的肿大胸腺。肿大胸腺是否占据双侧胸腔及胸腺大小并非胸腔镜手术的绝对禁忌证。该方法对患者安全、可行且微创。