Lindemann Christoph Heinrich, Wenzel Andrea, Erger Florian, Middelmann Lea, Borde Julika, Hahnen Eric, Krauß Denise, Oehm Simon, Arjune Sita, Todorova Polina, Burgmaier Kathrin, Liebau Max Christoph, Grundmann Franziska, Beck Bodo B, Müller Roman-Ulrich
University of Cologne, Faculty of Medicine and University Hospital Cologne, Department 2 of Internal Medicine, Cologne, Germany.
Institute of Human Genetics, University Hospital Cologne, Faculty of Medicine, University of Cologne, Cologne, Germany.
Kidney Int Rep. 2022 Dec 28;8(3):455-466. doi: 10.1016/j.ekir.2022.12.025. eCollection 2023 Mar.
Autosomal-dominant polycystic kidney disease (ADPKD) is the most common genetic cause of kidney failure. Because of the heterogeneity in disease progression in ADPKD, parameters predicting future outcome are important. The disease-causing genetic variant is one of these parameters.
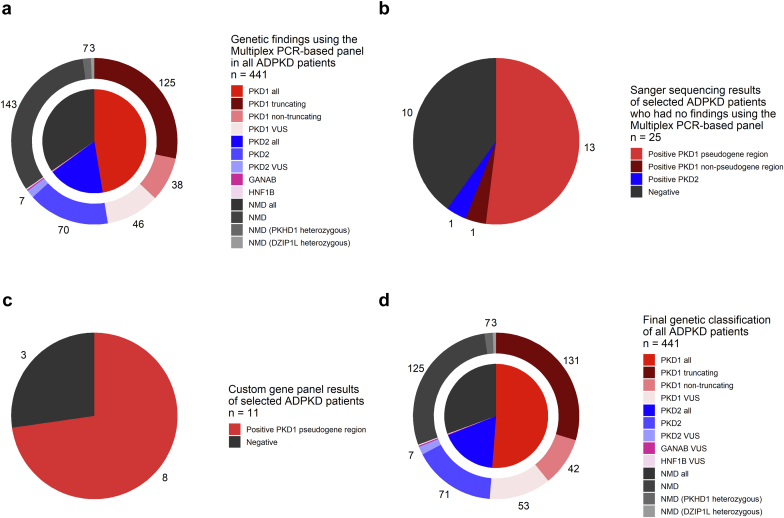
A multiplex polymerase chain reaction (PCR)-based panel (MPP) was established for analysis of 6 polycystic kidney disease (PKD) genes (, , , , and ) in 441 patients with ADPKD. Selected patients were additionally sequenced using Sanger sequencing or a custom enrichment-based gene panel. Results were combined with clinical characteristics to assess the impact of genetic data on clinical decision-making. Variants of unclear significance (VUS) were considered diagnostic based on a classic ADPKD clinical phenotype.
Using the MPP, disease-causing variants were detected in 65.3% of patients. Sanger sequencing and the custom gene panel in 32 patients who were MPP-negative revealed 20 variants missed by MPP, (estimated overall false negative rate 24.6%, false-positive rate 9.4%). Combining clinical and genetic data revealed that knowledge of the genotype could have impacted the treatment decision in 8.2% of patients with a molecular genetic diagnosis. Sequencing only the pseudogene homologous region in MPP-negative patients resulted in an acceptable false-negative rate of 3.28%.
The MPP yields rapid genotype information at lower costs and allows for simple extension of the panel for new disease genes. Additional sequencing of the pseudogene homologous region is required in negative cases. Access to genotype information even in settings with limited resources is important to allow for optimal patient counseling in ADPKD.
常染色体显性多囊肾病(ADPKD)是肾衰竭最常见的遗传病因。由于ADPKD疾病进展存在异质性,预测未来预后的参数很重要。致病基因变异就是这些参数之一。
建立了基于多重聚合酶链反应(PCR)的检测板(MPP),用于分析441例ADPKD患者的6个多囊肾病(PKD)基因(、、、、和)。对选定患者另外使用桑格测序或基于定制富集的基因检测板进行测序。将结果与临床特征相结合,以评估遗传数据对临床决策的影响。根据经典ADPKD临床表型,将意义不明确的变异(VUS)视为诊断性变异。
使用MPP,在65.3%的患者中检测到致病变异。对32例MPP检测结果为阴性的患者进行桑格测序和定制基因检测板检测,发现了20个MPP遗漏的变异(估计总体假阴性率为24.6%,假阳性率为9.4%)。结合临床和遗传数据显示,在8.2%的分子遗传学诊断患者中,基因型信息可能会影响治疗决策。仅对MPP阴性患者的假基因同源区域进行测序,假阴性率为3.28%,可接受。
MPP以较低成本产生快速的基因型信息,并允许简单扩展检测板以纳入新的疾病基因。阴性病例需要对假基因同源区域进行额外测序。即使在资源有限的情况下获取基因型信息,对于在ADPKD中进行最佳患者咨询也很重要。