University of Sousse, Faculty of Medicine of Sousse, 4002 Sousse, Tunisia; Farhat Hached University Hospital, Medical Intensive Care Unit, Research Laboratory "Heart Failure", LR12SP09, 4000 Sousse, Tunisia.
University of Sousse, Faculty of Medicine of Sousse, 4002 Sousse, Tunisia; Farhat Hached University Hospital, Medical Intensive Care Unit, Research Laboratory "Heart Failure", LR12SP09, 4000 Sousse, Tunisia.
J Infect Public Health. 2023 May;16(5):727-735. doi: 10.1016/j.jiph.2023.02.022. Epub 2023 Mar 10.
The worldwide SARS-CoV-2 pandemic represents the most recent global healthcare crisis. While all healthcare systems suffered facing the immense burden of critically-ill COVID-19 patients, the levels of preparedness and adaptability differed highly between countries.
to describe resource mobilization throughout the COVID-19 waves in Tunisian University Medical Intensive Care Units (MICUs) and to identify discrepancies in preparedness between the provided and required resource.
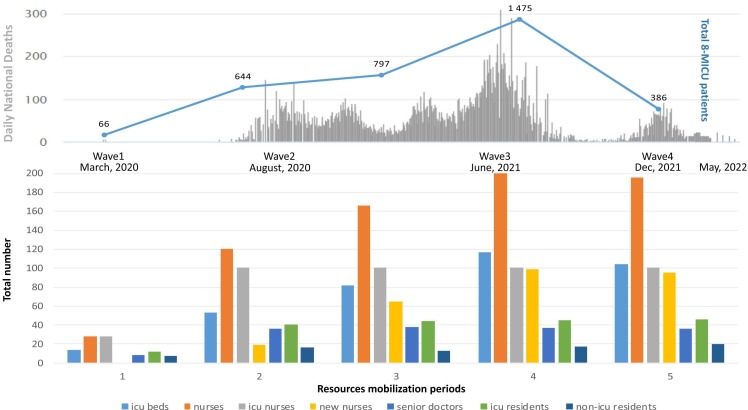
This is a longitudinal retrospective multicentre observational study conducted between March 2020 and May 2022 analyzing data from eight University MICUs. Data were collected at baseline and at each bed expansion period in relation to the nation's four COVID-19 waves. Data collected included epidemiological, organizational and management trends and outcomes of COVID-19 and non-COVID-19 admissions.
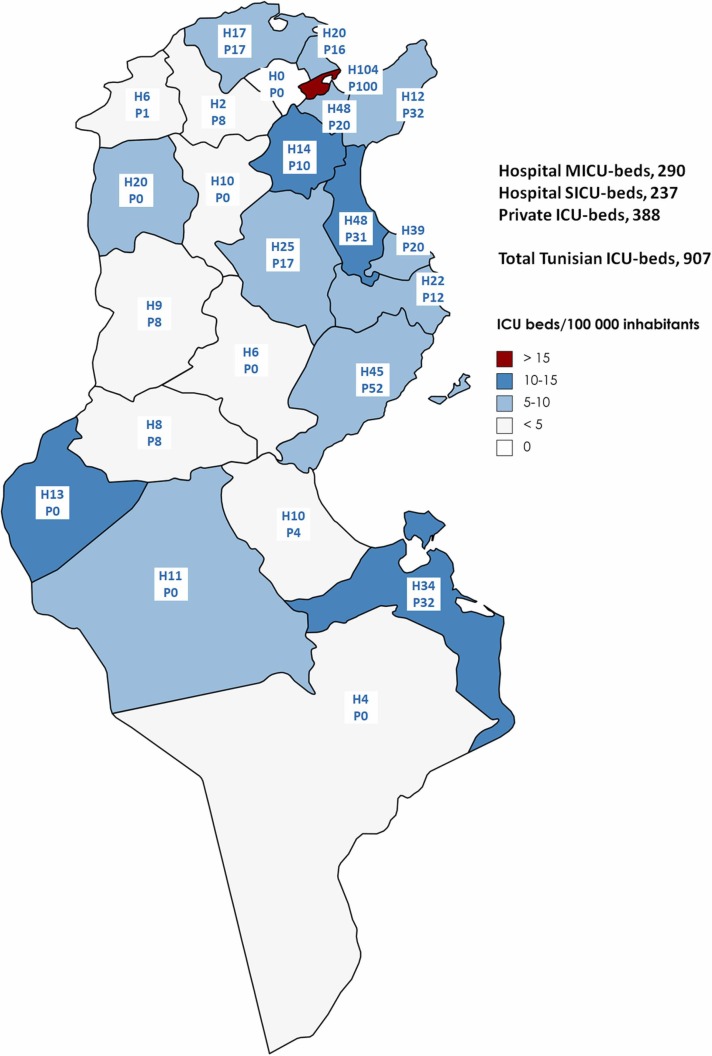
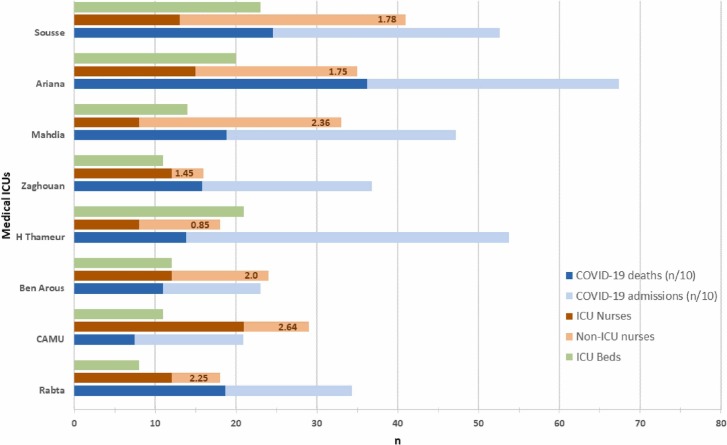
MICU-beds increased from 66 to a maximum of 117 beds. This was possible thanks to equipping pre-existing non-functional MICU beds (n = 20) and creating surge ICU-beds in medical wards (n = 24). MICU nurses increased from 53 to 200 of which 99 non-ICU nurses, by deployment from other departments and temporary recruitment. The nurse-to-MICU-bed ratio increased from 1:1 to around 1·8:1. Only 55% of beds were single rooms, 80% were equipped with ICU ventilators. These MICUs managed to admit a total of 3368 critically-ill patients (15% of hospital admissions). 33·2% of COVID-19-related intra-hospital deaths occurred within the MICUs.
Despite a substantial increase in resource mobilization during the COVID-19 pandemic, the current study identified significant persisting discrepancies between supplied and required resource, at least partially explaining the poor overall prognosis of critically-ill COVID-19 patients.
全球范围内的 SARS-CoV-2 大流行是最近一次全球医疗保健危机。虽然所有医疗保健系统在面对大量 COVID-19 重症患者时都承受了巨大的负担,但各国的准备水平和适应能力差异很大。
描述突尼斯大学重症监护病房(MICU)在 COVID-19 波次期间的资源调动情况,并确定提供资源与所需资源之间的差异。
这是一项纵向回顾性多中心观察性研究,于 2020 年 3 月至 2022 年 5 月期间在 8 所大学 MICU 进行,分析了与国家 COVID-19 四次波次相关的数据。数据在基线和每次床位扩张期间收集,包括 COVID-19 和非 COVID-19 入院的流行病学、组织和管理趋势以及结果。
MICU 床位从 66 张增加到最多 117 张。这得益于配备了以前未使用的非功能 MICU 床位(n=20)和在医疗病房创建了紧急 ICU 床位(n=24)。MICU 护士从 53 名增加到 200 名,其中 99 名非 ICU 护士是从其他部门部署和临时招聘而来的。护士与 MICU 床位的比例从 1:1 增加到 1.8:1 左右。只有 55%的床位是单人房,80%配备了 ICU 呼吸机。这些 MICU 总共收治了 3368 名重症患者(占医院入院人数的 15%)。COVID-19 相关院内死亡中有 33.2%发生在 MICU 内。
尽管在 COVID-19 大流行期间大量增加了资源调动,但本研究发现,提供的资源与所需资源之间仍存在显著差异,这至少部分解释了 COVID-19 重症患者总体预后较差的原因。