Persson Gustav, Lodin-Sundström Angelica, Linér Mats H, Andersson Samuel H A, Sjögreen Bodil, Andersson Johan P A
Department of Experimental Medical Science, Lund University, Lund, Sweden.
Department of Health Sciences, Mid Sweden University, Sundsvall, Sweden.
Front Physiol. 2023 Mar 7;14:1109958. doi: 10.3389/fphys.2023.1109958. eCollection 2023.
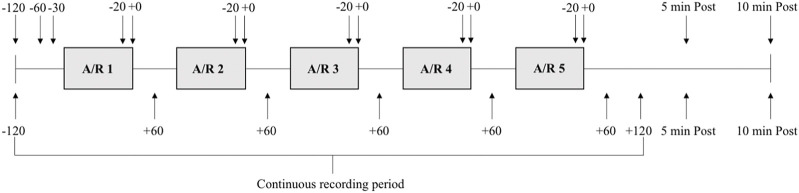
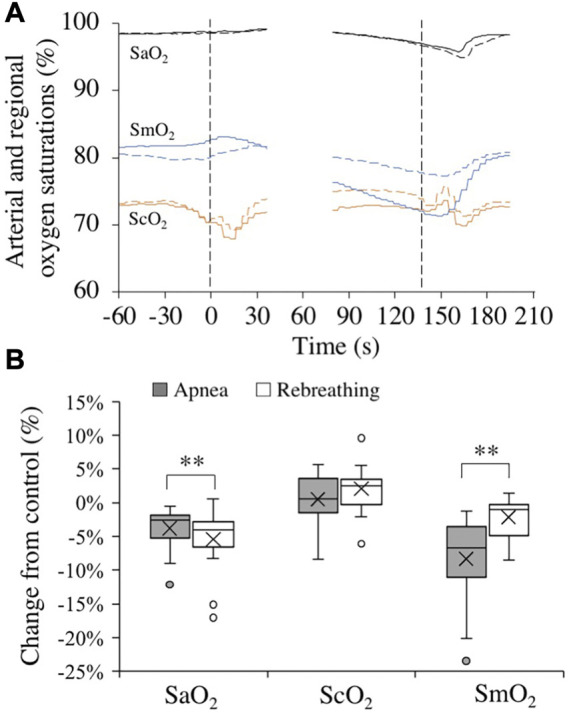
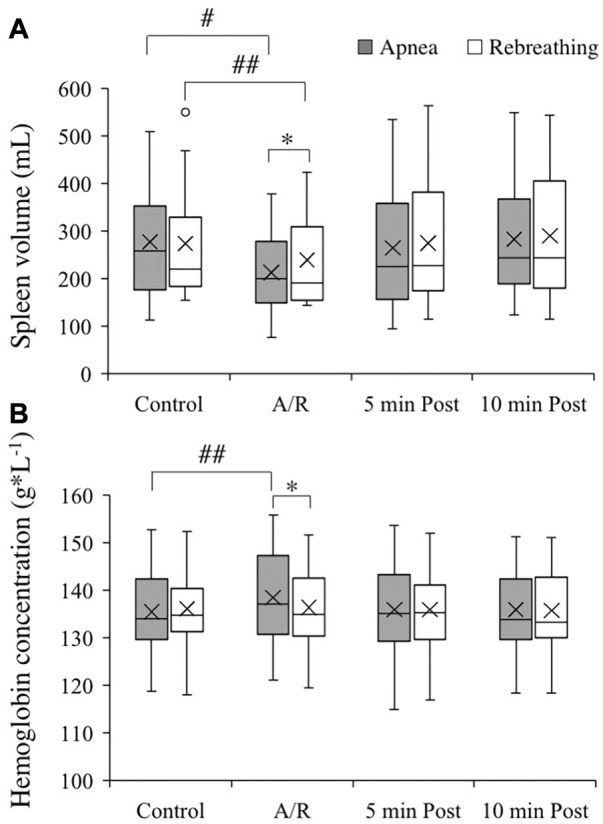
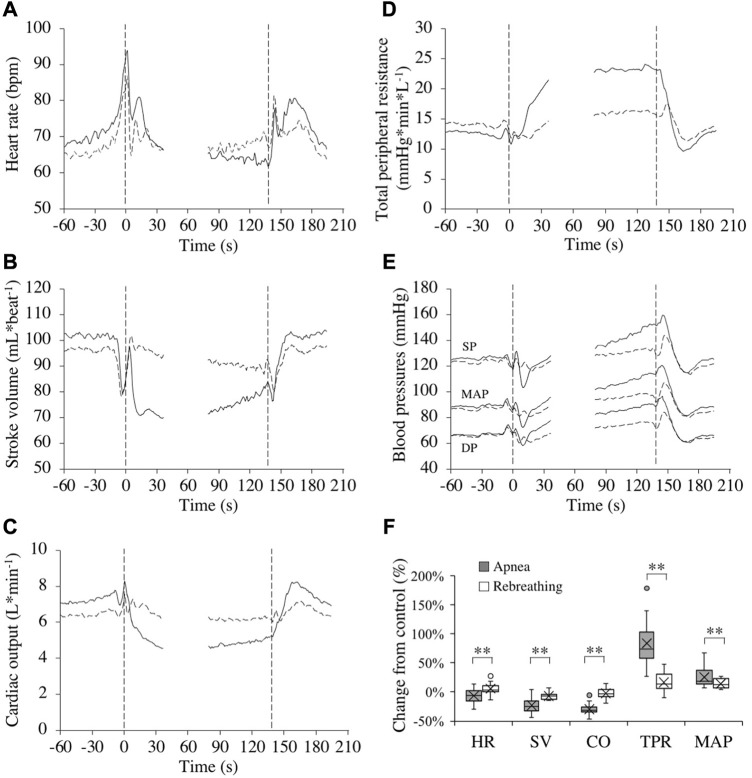
The spleen contracts during apnea, releasing stored erythrocytes, thereby increasing systemic hemoglobin concentration (Hb). We compared apnea and rebreathing periods, of equal sub-maximal duration (mean 137 s; SD 30), in eighteen subjects to evaluate whether respiratory arrest or hypoxic and hypercapnic chemoreceptor stimulation is the primary elicitor of splenic contraction and cardiovascular responses during apnea. Spleen volume, Hb, cardiovascular variables, arterial (SaO), cerebral (ScO), and deltoid muscle oxygen saturations (SmO) were recorded during the trials and end-tidal partial pressure of oxygen (PO) and carbon dioxide (PCO) were measured before and after maneuvers. The spleen volume was smaller after apnea, 213 (89) mL, than after rebreathing, 239 (95) mL, corresponding to relative reductions from control by 20.8 (17.8) % and 11.6 (8.0) %, respectively. The Hb increased 2.4 (2.0) % during apnea, while there was no significant change with rebreathing. The cardiovascular responses, including bradycardia, decrease in cardiac output, and increase in total peripheral resistance, were augmented during apnea compared to during rebreathing. The PO was higher, and the PCO was lower, after apnea compared to after rebreathing. The ScO was maintained during maneuvers. The SaO decreased 3.8 (3.1) % during apnea, and even more, 5.4 (4.4) %, during rebreathing, while the SmO decreased less during rebreathing, 2.2 (2.8) %, than during apnea, 8.3 (6.2) %. We conclude that respiratory arrest is an important stimulus for splenic contraction and Hb increase during apnea, as well as an important initiating factor for the apnea-associated cardiovascular responses and their oxygen-conserving effects.
在呼吸暂停期间脾脏会收缩,释放储存的红细胞,从而增加全身血红蛋白浓度(Hb)。我们比较了18名受试者在同等次最大持续时间(平均137秒;标准差30)的呼吸暂停期和再呼吸期,以评估呼吸停止或低氧和高碳酸血症化学感受器刺激是否是呼吸暂停期间脾脏收缩和心血管反应的主要诱发因素。在试验过程中记录脾脏体积、Hb、心血管变量、动脉血氧饱和度(SaO)、脑血氧饱和度(ScO)和三角肌肌肉血氧饱和度(SmO),并在操作前后测量呼气末氧分压(PO)和二氧化碳分压(PCO)。呼吸暂停后脾脏体积为213(89)毫升,小于再呼吸后的239(95)毫升,分别相对于对照减少了20.8(17.8)%和11.6(8.0)%。呼吸暂停期间Hb增加了2.4(2.0)%,而再呼吸期间无显著变化。与再呼吸期间相比,呼吸暂停期间包括心动过缓、心输出量减少和总外周阻力增加在内的心血管反应增强。与再呼吸后相比,呼吸暂停后PO更高,PCO更低。操作过程中ScO保持不变。呼吸暂停期间SaO下降了3.8(3.1)%,再呼吸期间下降得更多,为5.4(4.4)%,而SmO在再呼吸期间下降幅度小于呼吸暂停期间,分别为2.2(2.8)%和8.3(6.2)%。我们得出结论,呼吸停止是呼吸暂停期间脾脏收缩和Hb增加的重要刺激因素,也是与呼吸暂停相关的心血管反应及其氧保存作用的重要起始因素。