Hakim Shariful, Chowdhury Muhammad Abdul Baker, Haque Md Ashiqul, Ahmed Nasar U, Paul Gowranga Kumar, Uddin Md Jamal
Department of Statistics, Shahjalal University of Science & Technology, Sylhet, Bangladesh.
Chander Hat Degree College, Nilphamari, Bangladesh.
PLOS Glob Public Health. 2022 Nov 28;2(11):e0001154. doi: 10.1371/journal.pgph.0001154. eCollection 2022.
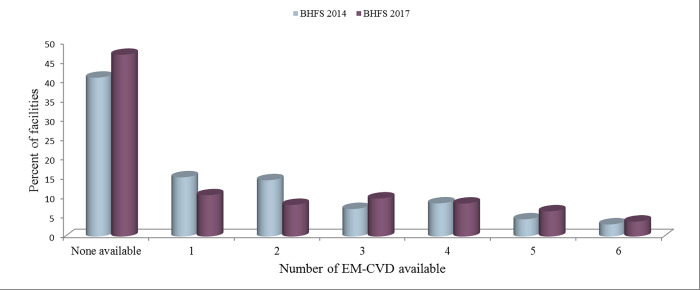
Long-term, often lifelong care for cardiovascular disease (CVD) patients requires consistent use of medicine; hence, the availability of essential medicine for CVD (EM-CVD) is vital for treatment, quality of life, and survival. We aimed to assess the availability of EM-CVD and explore healthcare facility (HCF) characteristics associated with the availability of those medicines in Bangladesh. This study utilized publicly available cross-sectional data from the 2014 and 2017 waves of the Bangladesh Health Facilities Survey (BHFS). The analysis included 204 facilities (84 from the 2014 BHFS and 120 from the 2017 BHFS) that provide CVD diagnosis and treatment services. The outcome variable "EM-CVD availability" was calculated as a counting score of the following tracer medicines: angiotensin-converting enzyme (ACE) inhibitors (enalapril), thiazide, beta-blockers (atenolol), calcium channel blockers (amlodipine and nifedipine), aspirin, and simvastatin/atorvastatin. A multivariable Poisson regression model was used to identify the HCF characteristics associated with EM-CVD availability. The number of Bangladeshi HCFs that provide CVD screening and treatment services increased just a little between 2014 and 2017 (from 5.4% to 7.9%). Since 2014, there has been an increase in the availability of calcium channel blockers (from 37.5% to 38.5%), aspirin (from 25.3% to 27.9%), and simvastatin/atorvastatin (from 8.0% to 30.7%), whereas there has been a decrease in the availability of ACE inhibitors (enalapril) (from 12.5% to 6.5%), thiazide (from 15.7% to 11.1%), and beta-blockers (from 42.5% to 32.5%). The likelihood of EM-CVD being available was higher among private and urban facilities than among public and rural facilities. Furthermore, facilities that had 24-hour staff coverage and performed quality assurance activities had a higher chance of having EM-CVD available than those that did not have 24-hour staff coverage and did not undertake quality assurance activities. Government authorities should think about a wide range of policy implications, such as putting more emphasis on public and rural facilities, making sure staff is available 24 hours a day, and performing quality assurance activities at facilities to make EM-CVD more available.
心血管疾病(CVD)患者的长期护理,通常是终身护理,需要持续用药;因此,心血管疾病基本药物(EM-CVD)的可及性对于治疗、生活质量和生存至关重要。我们旨在评估EM-CVD的可及性,并探讨与孟加拉国这些药物可及性相关的医疗机构(HCF)特征。本研究利用了来自孟加拉国卫生设施调查(BHFS)2014年和2017年两轮公开的横断面数据。分析纳入了204家提供CVD诊断和治疗服务的机构(2014年BHFS中的84家以及2017年BHFS中的120家)。结果变量“EM-CVD可及性”通过以下示踪药物的计数得分来计算:血管紧张素转换酶(ACE)抑制剂(依那普利)、噻嗪类、β受体阻滞剂(阿替洛尔)、钙通道阻滞剂(氨氯地平和硝苯地平)、阿司匹林以及辛伐他汀/阿托伐他汀。使用多变量泊松回归模型来确定与EM-CVD可及性相关的HCF特征。2014年至2017年期间,孟加拉国提供CVD筛查和治疗服务的HCF数量仅略有增加(从5.4%增至7.9%)。自2014年以来,钙通道阻滞剂的可及性有所增加(从37.5%增至38.5%)、阿司匹林(从25.3%增至27.9%)以及辛伐他汀/阿托伐他汀(从8.0%增至30.7%),而ACE抑制剂(依那普利)的可及性有所下降(从12.5%降至6.5%)、噻嗪类(从15.7%降至11.1%)以及β受体阻滞剂(从42.5%降至32.5%)。私立和城市医疗机构中EM-CVD可及的可能性高于公立和农村医疗机构。此外,有24小时工作人员值班且开展质量保证活动的机构,其EM-CVD可及的机会高于没有24小时工作人员值班且未开展质量保证活动的机构。政府当局应考虑一系列政策影响,例如更加重视公立和农村医疗机构、确保每天24小时都有工作人员值班,以及在各机构开展质量保证活动,以使EM-CVD更易获得。