Diamond-Smith Nadia G, Sharma Preetika, Duggal Mona, Gill Navneet, Gupta Jagriti, Kumar Vijay, Kaur Jasmeet, Singh Pushpendra, Vosburg Katy Bradford, El Ayadi Alison M
University of California, San Francisco, CA, United States of America.
Post Graduate Institute of Medical Education and Research, Chandigarh, India.
PLOS Glob Public Health. 2022 Dec 6;2(12):e0001321. doi: 10.1371/journal.pgph.0001321. eCollection 2022.
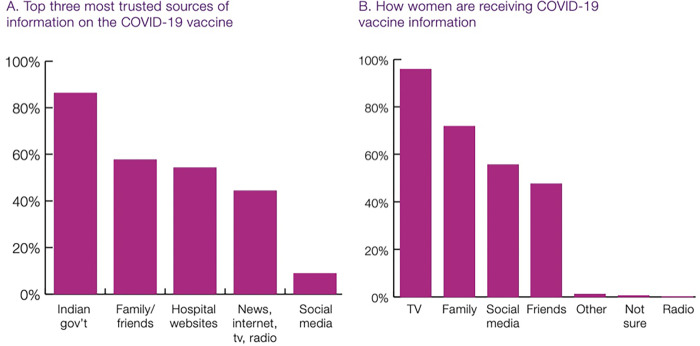
Despite COVID-19 vaccines being available to pregnant women in India since summer 2021, little is known about vaccine uptake among this high need population. We conducted mixed methods research with pregnant and recently delivered rural women in northern India, consisting of 300 phone surveys and 15 in-depth interviews, in November 2021. Only about a third of respondents were vaccinated, however, about half of unvaccinated respondents reported that they would get vaccinated now if they could. Fears of harm to the unborn baby or young infant were common (22% of unvaccinated women). However, among unvaccinated women who wanted to get vaccinated, the most common barrier reported was that their health care provider refused to provide them the vaccine. Gender barriers and social norms also played a role, with family members restricting women's access. Trust in the health system was high, however, women were most often getting information about COVID-19 vaccines from sources that they did not trust, and they knew they were getting potentially poor-quality information. Qualitative data shed light on the barriers women faced from their family and health care providers but described how as more people got the vaccine that norms were changing. These findings highlight how pregnant women in India have lower vaccination rates than the general population, and while vaccine hesitancy does play a role, structural barriers from the health care system also limit access to vaccines. Interventions must be developed that target household decision-makers and health providers at the community level, and that take advantage of the trust that rural women already have in their health care providers and the government. It is essential to think beyond vaccine hesitancy and think at the system level when addressing this missed opportunity to vaccinate high risk pregnant women in this setting.
自2021年夏季起,印度就已向孕妇提供新冠疫苗,但对于这一高需求人群的疫苗接种情况却知之甚少。2021年11月,我们对印度北部农村地区的孕妇及刚分娩的妇女开展了混合方法研究,包括300次电话调查和15次深度访谈。只有约三分之一的受访者接种了疫苗,然而,约一半未接种的受访者表示,如果可以的话,她们现在会接种疫苗。担心对未出生的婴儿或幼儿造成伤害的情况很常见(22%的未接种疫苗的女性)。然而,在想要接种疫苗的未接种疫苗的女性中,最常见的障碍是她们的医疗保健提供者拒绝为她们提供疫苗。性别障碍和社会规范也起到了作用,家庭成员限制了女性获取疫苗的机会。对卫生系统的信任度很高,然而,女性获取新冠疫苗信息的来源往往是她们不信任的,而且她们知道自己得到的可能是质量不佳的信息。定性数据揭示了女性在家庭和医疗保健提供者方面面临的障碍,但也描述了随着越来越多的人接种疫苗,规范正在发生变化。这些发现凸显出印度孕妇的疫苗接种率低于普通人群,虽然疫苗犹豫确实起到了一定作用,但医疗保健系统的结构性障碍也限制了疫苗的获取。必须制定针对家庭决策者和社区层面医疗服务提供者的干预措施,并利用农村女性对其医疗保健提供者和政府已有的信任。在解决这一错失为该地区高危孕妇接种疫苗机会的问题时,至关重要的是要超越疫苗犹豫,从系统层面进行思考。