Miyamoto Yasunori, Honda Akira, Yokose Seiji, Nagata Mariko, Miyamoto Jiro
Division of Internal Medicine, Miyamoto Hospital, Inashiki 300-0605, Ibaraki, Japan.
Division of Gastroenterology and Hepatology, Tokyo Medical University Ibaraki Medical Center, Ami 300-0395, Ibaraki, Japan.
J Clin Med. 2023 Mar 14;12(6):2253. doi: 10.3390/jcm12062253.
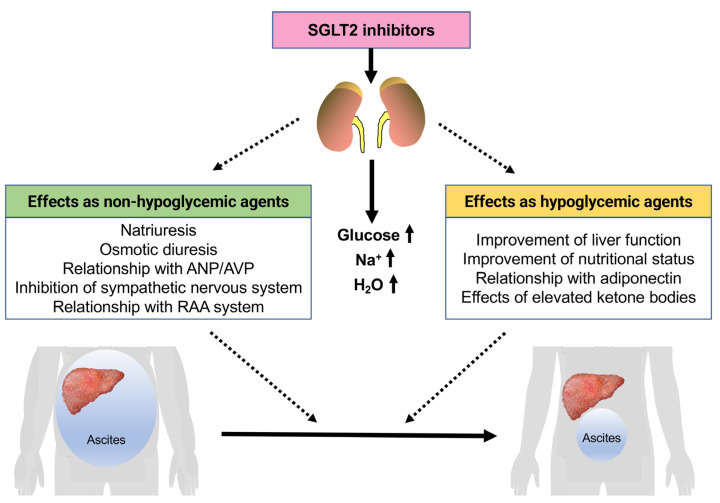
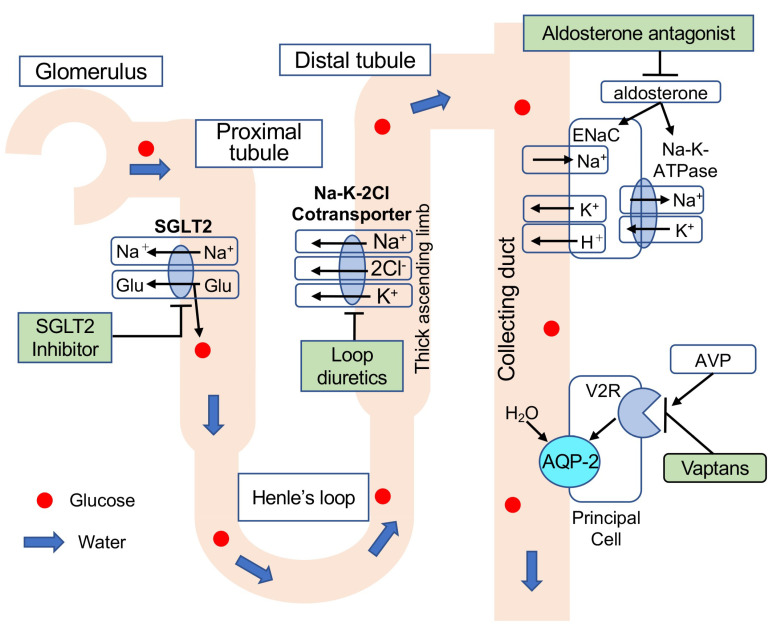
Decompensated liver cirrhosis is often complicated by refractory ascites, and intractable ascites are a predictor of poor prognosis in patients with liver cirrhosis. The treatment of ascites in patients with cirrhosis is based on the use of aldosterone blockers and loop diuretics, and occasionally vasopressin receptor antagonists are also used. Recent reports suggest that sodium-glucose cotransporter 2 (SGLT2) inhibitors may be a new treatment for refractory ascites with a different mechanism with respect to conventional agents. The main mechanisms of ascites reduction with SGLT2 inhibitors appear to be natriuresis and osmotic diuresis. However, other mechanisms, including improvements in glucose metabolism and nutritional status, hepatoprotection by ketone bodies and adiponectin, amelioration of the sympathetic nervous system, and inhibition of the renin-angiotensin-aldosterone system, may also contribute to the reduction of ascites. This literature review describes previously reported cases in which SGLT2 inhibitors were used to effectively treat ascites caused by liver cirrhosis. The discussion of the mechanisms involved is expected to contribute to establishing SGLT2 therapy for ascites in the future.
失代偿期肝硬化常并发难治性腹水,而顽固性腹水是肝硬化患者预后不良的一个预测指标。肝硬化患者腹水的治疗基于使用醛固酮受体阻滞剂和袢利尿剂,偶尔也会使用血管加压素受体拮抗剂。最近的报告表明,钠-葡萄糖协同转运蛋白2(SGLT2)抑制剂可能是一种治疗难治性腹水的新方法,其作用机制与传统药物不同。SGLT2抑制剂减少腹水的主要机制似乎是利钠和渗透性利尿。然而,其他机制,包括改善糖代谢和营养状况、酮体和脂联素的肝脏保护作用、交感神经系统的改善以及肾素-血管紧张素-醛固酮系统的抑制,也可能有助于减少腹水。这篇文献综述描述了先前报道的使用SGLT2抑制剂有效治疗肝硬化引起的腹水的病例。对所涉及机制的讨论有望为未来建立SGLT2治疗腹水的方法做出贡献。