Department of Cardiology and Angiology, BG University Hospital Bergmannsheil, Ruhr-Universität Bochum, Bürkle-de-La-Camp-Platz 1, 44789, Bochum, Germany.
Institute for Prevention and Occupational Medicine of the German Social Accident Insurance, Institute of the Ruhr-Universität Bochum (IPA), Bochum, Germany.
Sci Rep. 2023 Mar 29;13(1):5143. doi: 10.1038/s41598-023-31944-7.
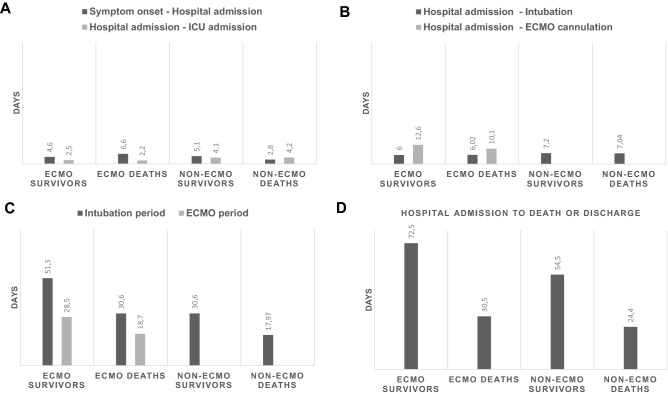
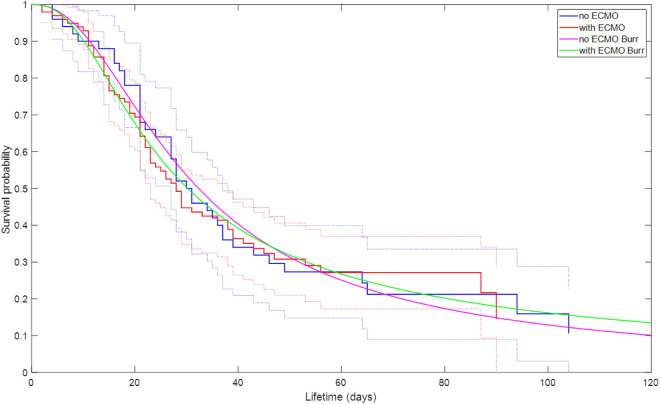
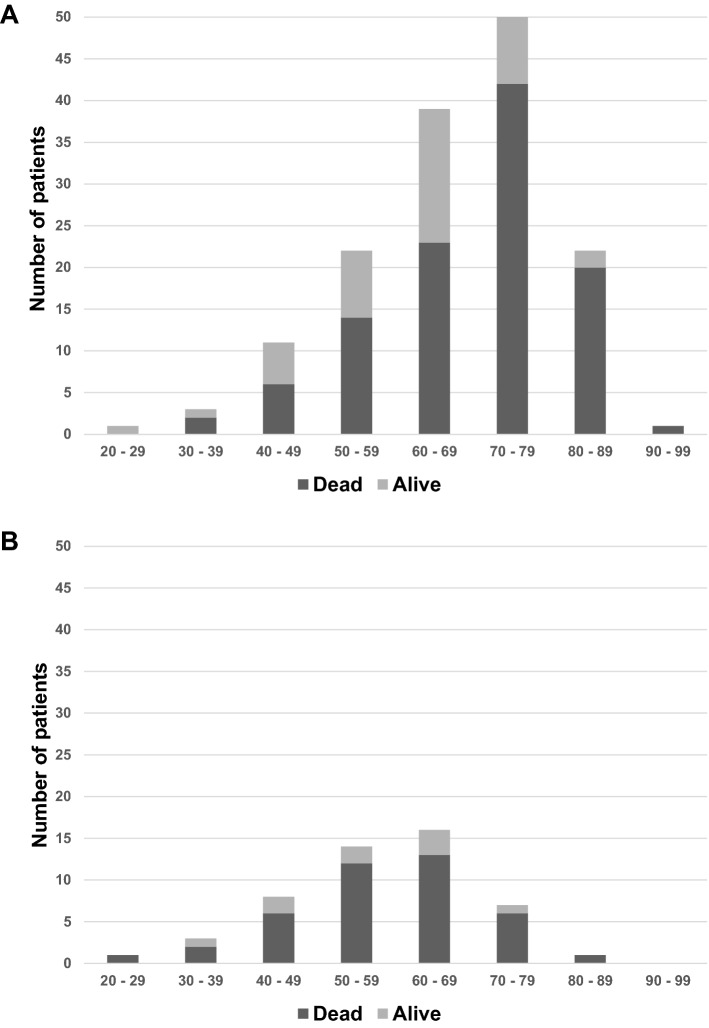
The use of extracorporeal membrane oxygenation (ECMO) is discussed to improve patients' outcome in severe COVID-19 with respiratory failure, but data on ECMO remains controversial. The aim of the study was to determine the characteristics of patients under invasive mechanical ventilation (IMV) with or without veno-venous ECMO support and to evaluate outcome parameters. Ventilated patients with COVID-19 with and without additional ECMO support were analyzed in a retrospective multicenter study regarding clinical characteristics, respiratory and laboratory parameters in day-to-day follow-up. Recruitment of patients was conducted during the first three COVID-19 waves at four German university hospitals of the Ruhr University Bochum, located in the Middle Ruhr Region. From March 1, 2020 to August 31, 2021, the charts of 149 patients who were ventilated for COVID-19 infection, were included (63.8% male, median age 67 years). Fifty patients (33.6%) received additional ECMO support. On average, ECMO therapy was initiated 15.6 ± 9.4 days after symptom onset, 10.6 ± 7.1 days after hospital admission, and 4.8 ± 6.4 days after the start of IMV. Male sex and higher SOFA and RESP scores were observed significantly more often in the high-volume ECMO center. Pre-medication with antidepressants was more often detected in survivors (22.0% vs. 6.5%; p = 0.006). ECMO patients were 14 years younger and presented a lower rate of concomitant cardiovascular diseases (18.0% vs. 47.5%; p = 0.0004). Additionally, cytokine-adsorption (46.0% vs. 13.1%; p < 0.0001) and renal replacement therapy (76.0% vs. 43.4%; p = 0.0001) were carried out more frequently; in ECMO patients thrombocytes were transfused 12-fold more often related to more than fourfold higher bleeding complications. Undulating C-reactive protein (CRP) and massive increase in bilirubin levels (at terminal stage) could be observed in deceased ECMO patients. In-hospital mortality was high (Overall: 72.5%, ECMO: 80.0%, ns). Regardless of ECMO therapy half of the study population deceased within 30 days after hospital admission. Despite being younger and with less comorbidities ECMO therapy did not improve survival in severely ill COVID-19 patients. Undulating CRP levels, a massive increase of bilirubin level and a high use of cytokine-adsorption were associated with worse outcomes. In conclusion, ECMO support might be helpful in selected severe cases of COVID-19.
体外膜肺氧合(ECMO)的使用被讨论用于改善严重 COVID-19 伴呼吸衰竭患者的预后,但 ECMO 的数据仍存在争议。本研究的目的是确定接受有创机械通气(IMV)加或不加静脉-静脉 ECMO 支持患者的特征,并评估预后参数。在一项回顾性多中心研究中,对伴有或不伴有额外 ECMO 支持的 COVID-19 呼吸机患者进行分析,以评估临床特征、每日随访中的呼吸和实验室参数。该研究在德国鲁尔大学波鸿分校的四所大学医院进行,这些医院位于米德兰鲁尔地区。2020 年 3 月 1 日至 2021 年 8 月 31 日,纳入了 149 名因 COVID-19 感染而接受通气的患者(63.8%为男性,中位年龄 67 岁)。50 名患者(33.6%)接受了额外的 ECMO 支持。平均而言,ECMO 治疗在症状出现后 15.6±9.4 天、入院后 10.6±7.1 天和 IMV 开始后 4.8±6.4 天开始。在大容量 ECMO 中心,男性和更高的 SOFA 和 RESP 评分更常见。幸存者中更常发现抗抑郁药治疗(22.0% vs. 6.5%;p=0.006)。ECMO 患者年轻 14 岁,合并心血管疾病的发生率较低(18.0% vs. 47.5%;p=0.0004)。此外,细胞因子吸附(46.0% vs. 13.1%;p<0.0001)和肾脏替代治疗(76.0% vs. 43.4%;p=0.0001)更为常见;ECMO 患者的血小板输注量增加了 12 倍,出血并发症增加了 4 倍以上。在死亡的 ECMO 患者中可以观察到 CRP 水平波动和胆红素水平大量增加(终末期)。院内死亡率很高(总体:72.5%,ECMO:80.0%,无差异)。无论是否进行 ECMO 治疗,研究人群中有一半在入院后 30 天内死亡。尽管 ECMO 治疗的患者更年轻且合并症较少,但并未改善严重 COVID-19 患者的生存。CRP 水平波动、胆红素水平大量增加和细胞因子吸附的大量使用与预后不良相关。总之,ECMO 支持可能对 COVID-19 的某些严重病例有益。