Luo Mian-Na, Pan Qingjun, Ye Ting, Li Shangmei, Yang Lawei, Liu Hua-Feng, Xu Yongzhi
Guangdong Provincial Key Laboratory of Autophagy and Major Chronic Non-Communicable Diseases, Affiliated Hospital of Guangdong Medical University, Zhanjiang, China.
Department of Nephrology, Affiliated Hospital of Guangdong Medical University, Zhanjiang, China.
Front Pharmacol. 2023 Mar 14;14:1093442. doi: 10.3389/fphar.2023.1093442. eCollection 2023.
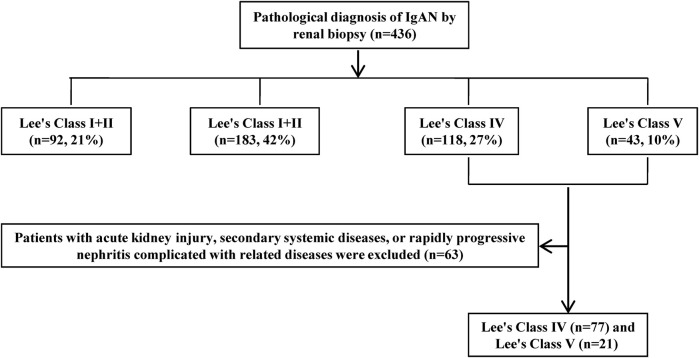
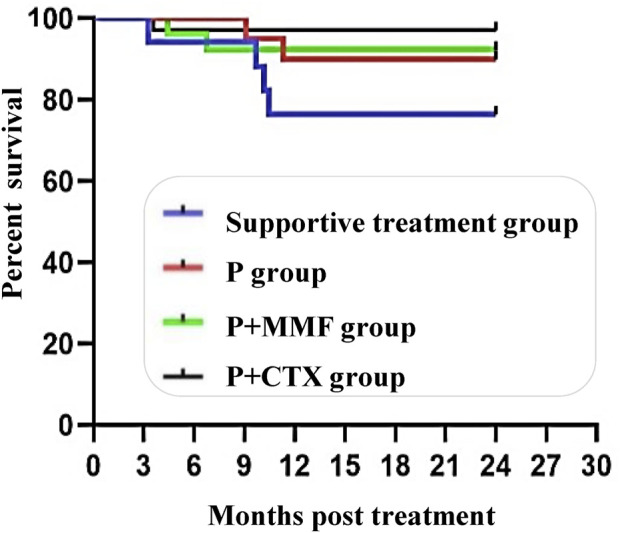
This study compared the efficacy and safety of sequential immunosuppressive therapy in patients with non-end-stage IgA nephropathy (IgAN) with Lee's classification of IV ∼ V and provided evidence for the use of immunotherapy in patients with severe IgAN. We retrospectively analyzed the clinical data of patients with Lee's IV ∼ V non-end-stage IgA nephropathy. 436 patients were diagnosed with IgAN, and 98 patients who met the inclusion criteria were included in this retrospective study. Of these, 17 were in the supportive care group, 20 in the P group (prednisone-only), 35 in P + CTX group (the prednisone combined with cyclophosphamide followed by mycophenolate mofetil), and 26 in the P + MMF group (prednisone combined with mycophenolate mofetil). The four groups showed differences in the segmental glomerulosclerosis score and the proportion of patients with Lee's grade IV ( < 0.05), but no differences in other indicators. Compared with the baseline values, urine protein-to-creatinine ratio (PCR) significantly decreased and serum albumin increased ( < 0.05), but there was no significant difference between the groups. The estimated Glomerular Filtration Rate (eGFR) of the P, P + MMF, and P + CTX groups were higher than that of the supportive care group at the 6th and 24th month after treatment (all < 0.05). At the 24th month, the eGFR in the P + CTX group was higher than that in the P + MMF group ( < 0.05). The effective remission rate of the P + CTX group was higher than that of the supportive care group ( < 0.05). At 12 months, the effective remission rate of the P group was higher than that of the supportive care group ( < 0.05). At the 24th month, there was no significant difference in the effective remission rates among the three groups (P, P + MMF, and P + CTX). Nine patients with severe IgA nephropathy reached the endpoint. This study showed that immunosuppressive therapy insevere IgAN patient scan effectively reduce urinary protein, increase albumin, and protect renal function in the early stages of IgAN. P + CTX is the most commonly used, which has a high effective remission rate of urine protein and a low incidence of end-point events.
本研究比较了序贯免疫抑制疗法对Lee氏分级为IV~V级的非终末期IgA肾病(IgAN)患者的疗效和安全性,并为重症IgA肾病患者免疫治疗的应用提供了依据。我们回顾性分析了Lee氏IV~V级非终末期IgA肾病患者的临床资料。436例患者被诊断为IgA肾病,98例符合纳入标准的患者被纳入本回顾性研究。其中,17例在支持治疗组,20例在P组(仅用泼尼松),35例在P+CTX组(泼尼松联合环磷酰胺后用霉酚酸酯),26例在P+MMF组(泼尼松联合霉酚酸酯)。四组在节段性肾小球硬化评分和Lee氏IV级患者比例方面存在差异(<0.05),但在其他指标上无差异。与基线值相比,尿蛋白肌酐比值(PCR)显著降低,血清白蛋白升高(<0.05),但组间无显著差异。治疗后第6个月和第24个月,P组、P+MMF组和P+CTX组的估计肾小球滤过率(eGFR)高于支持治疗组(均<0.05)。在第24个月时,P+CTX组的eGFR高于P+MMF组(<0.05)。P+CTX组的有效缓解率高于支持治疗组(<0.05)。在12个月时,P组的有效缓解率高于支持治疗组(<0.05)。在第24个月时,三组(P组、P+MMF组和P+CTX组)的有效缓解率无显著差异。9例重症IgA肾病患者达到终点。本研究表明,免疫抑制治疗在重症IgA肾病患者中可有效降低尿蛋白、增加白蛋白,并在IgA肾病早期保护肾功能。P+CTX是最常用的,其尿蛋白有效缓解率高,终点事件发生率低。