Departments of Oral and Maxillofacial-Head and Neck Oncology.
Oral Pathology.
Int J Surg. 2023 Apr 1;109(4):879-886. doi: 10.1097/JS9.0000000000000353.
Surgery and postoperative adjuvant therapy comprise the standard treatment for locally advanced resectable oral squamous cell carcinoma (LAROSCC), while preoperative neoadjuvant therapy is being explored without sufficient confirmation of improved survival. De-escalation regimens after neoadjuvant therapy, such as those omitting adjuvant radiotherapy, may provide comparable or better outcomes, suggesting rigorous assessment of adjuvant therapy outcomes is needed in LAROSCC patients. The authors thus performed this retrospective study in LAROSCC patients who received neoadjuvant therapy and surgery, to compare the outcomes for overall survival (OS) and locoregional recurrence-free survival (LRFS) between the adjuvant radiotherapy (radio) and nonradiotherapy (nonradio) cohorts.
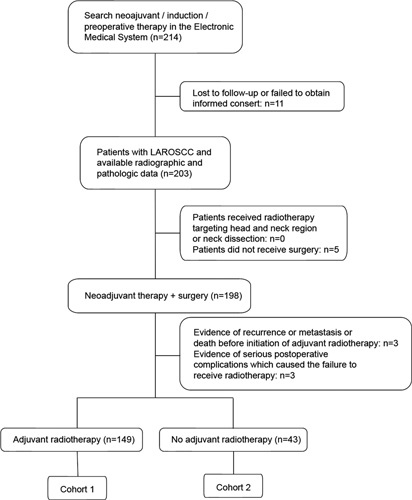
Patients diagnosed with LAROSCC who received neoadjuvant therapy and surgery were enrolled and divided into radio and nonradio cohorts to determine whether adjuvant radiotherapy could be omitted after neoadjuvant therapy and surgery.
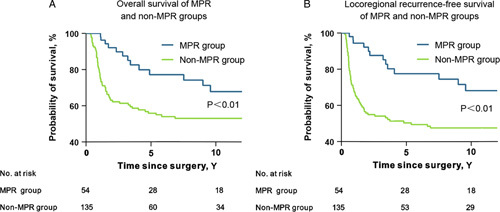
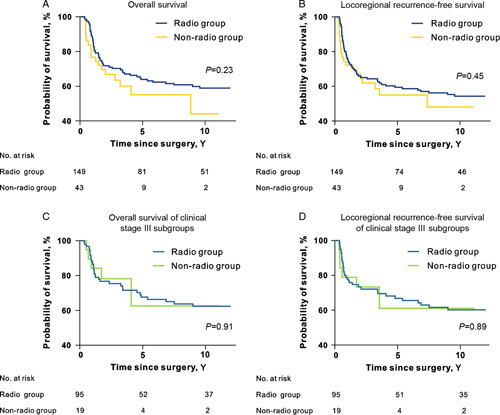
From 2008 to 2021, 192 patients were enrolled. No significant differences were found in OS or LRFS between the radio and nonradio patient cohorts. The 10-year estimated OS rates were 58.9 versus 44.1% in radio versus nonradio cohorts, while 10-year estimated LRFS rates were 55.4 versus 48.2%, respectively. For clinical stage III patients, 10-year OS rates were 62.3 versus 62.6% (radio vs. nonradio), and estimated 10-year LRFS rates were 56.5 versus 60.7% (radio vs. nonradio). Multivariate Cox regression modeling of postoperative variables showed pathologic response of primary tumor and pathologic regional lymph nodes staging were associated with survival, while the adjuvant radiotherapy exposure was not included in the model due to nonsignificance.
These findings support further prospective evaluation of adjuvant radiotherapy omission, and suggest that de-escalation trials are warranted for LAROSCC surgery patients who received neoadjuvant therapy.
手术和术后辅助治疗构成了局部晚期可切除口腔鳞状细胞癌(LAROSCC)的标准治疗方法,而新辅助治疗正在探索中,尚未充分证实其生存获益的改善。新辅助治疗后降级方案,如省略辅助放疗,可能提供相当或更好的结果,这表明需要对 LAROSCC 患者的辅助治疗结果进行严格评估。因此,作者在接受新辅助治疗和手术的 LAROSCC 患者中进行了这项回顾性研究,以比较辅助放疗(放疗)和非放疗(非放疗)队列的总生存(OS)和局部区域无复发生存(LRFS)结果。
入组并分为放疗和非放疗队列,以确定新辅助治疗和手术后是否可以省略辅助放疗。
2008 年至 2021 年,共纳入 192 例患者。放疗组和非放疗组患者的 OS 和 LRFS 无显著差异。放疗组和非放疗组的 10 年估计 OS 率分别为 58.9%和 44.1%,10 年估计 LRFS 率分别为 55.4%和 48.2%。对于临床分期 III 期患者,10 年 OS 率分别为 62.3%和 62.6%(放疗与非放疗),10 年估计 LRFS 率分别为 56.5%和 60.7%(放疗与非放疗)。术后变量的多变量 Cox 回归模型显示,原发肿瘤的病理反应和病理区域淋巴结分期与生存相关,而辅助放疗暴露由于无统计学意义未纳入模型。
这些发现支持进一步前瞻性评估辅助放疗的省略,并表明对于接受新辅助治疗的 LAROSCC 手术患者,需要进行降级试验。