Department of Clinical Sciences, Faculty of Medicine, University of Turku, Turku, Finland.
Department of Paediatrics and Adolescent Medicine, Turku University Hospital, Turku, Finland.
Pediatr Res. 2023 Oct;94(4):1480-1487. doi: 10.1038/s41390-023-02560-y. Epub 2023 Apr 5.
Preterm children with their aberrant gut microbiota and susceptibility to infections and inflammation constitute a considerable target group for probiotic therapy to generate the age-appropriate healthy microbiota.
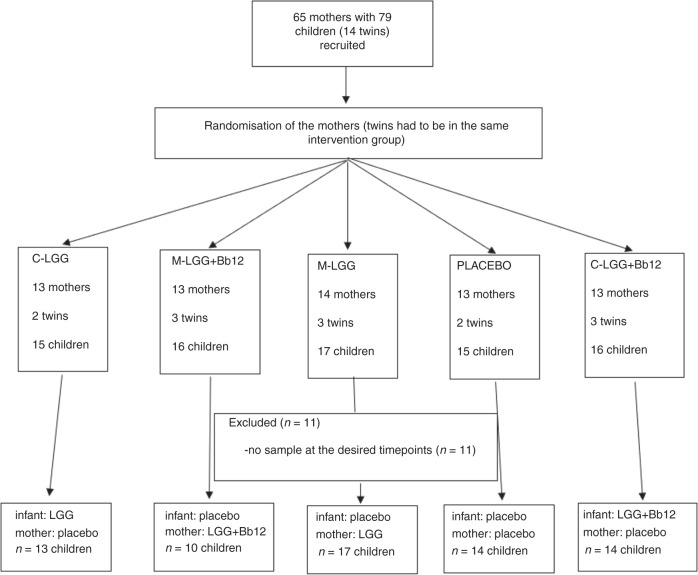
68 preterm neonates were randomized into five intervention groups: Beginning from the median age of 3 days, 13 children received Lactobacillus rhamnosus GG (LGG) directly orally, and 17 via the lactating mother. 14 children received LGG with Bifidobacterium lactis Bb-12 (Bb12) orally, and 10 via the lactating mother. 14 children received placebo. The children's faecal microbiota was assessed at the age of 7 days by 16S rRNA gene sequencing.
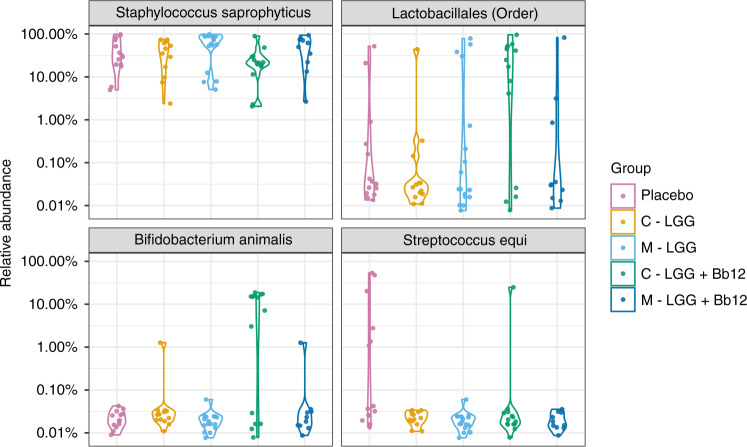
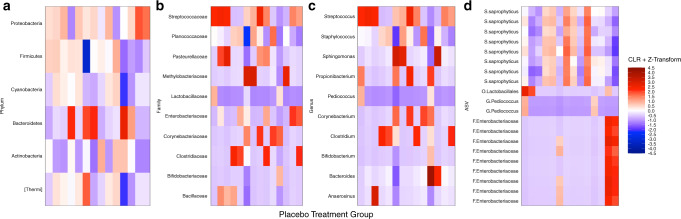
The gut microbiota compositions of the children directly receiving the probiotic combination (LGG + Bb12) were significantly different from those of the children receiving the other intervention modes or placebo (p = 0.0012; PERMANOVA), the distinction being due to an increase in the relative abundance of Bifidobacterium animalis (P < 0.00010; ANCOM-BC), and the order Lactobacillales (P = 0.020; ANCOM-BC).
The connection between aberrant primary gut microbiota and a heightened risk of infectious and non-communicable diseases invites effective microbiota modulation. We show that the direct, early, and brief probiotic intervention of LGG + Bb12 10 CFU each, is sufficient to modulate the gut microbiota of the preterm neonate.
Preterm children have a higher risk of several health problems partly due to their aberrant gut microbiota. More research is needed to find a safe probiotic intervention to modify the gut microbiota of preterm children. The maternal administration route via breast milk might be safer for the newborn. In our study, the early and direct administration of the probiotic combination Lactobacillus rhamnosus GG with Bifidobacterium lactis Bb-12 increased the proportion of bifidobacteria in the preterm children's gut at the age of 7 days, but the maternal administration route was not as effective.
早产儿的肠道微生物群异常,易受感染和炎症的影响,这使得他们成为益生菌治疗的重要目标群体,以产生适合年龄的健康微生物群。
将 68 名早产儿随机分为五组干预组:从中位数为 3 天的年龄开始,13 名儿童直接口服鼠李糖乳杆菌 GG(LGG),17 名儿童通过哺乳期母亲口服。14 名儿童口服含有双歧杆菌乳双歧杆菌 Bb-12(Bb12)的 LGG,10 名儿童通过哺乳期母亲口服。14 名儿童服用安慰剂。在 7 天时,通过 16S rRNA 基因测序评估儿童的粪便微生物群。
直接接受益生菌组合(LGG+Bb12)的儿童的肠道微生物群组成与接受其他干预模式或安慰剂的儿童有显著差异(p=0.0012;PERMANOVA),这种差异是由于双歧杆菌属动物双歧杆菌(Bifidobacterium animalis)相对丰度的增加(P<0.00010;ANCOM-BC)和乳杆菌目(Lactobacillales)的顺序(P=0.020;ANCOM-BC)。
异常的主要肠道微生物群与传染病和非传染性疾病的高风险之间存在联系,这就需要进行有效的微生物群调节。我们表明,直接、早期和简短的益生菌干预,LGG+Bb12 各 10CFU,足以调节早产儿的肠道微生物群。
早产儿由于其异常的肠道微生物群,存在多种健康问题的更高风险。需要更多的研究来寻找一种安全的益生菌干预措施来改变早产儿的肠道微生物群。通过母乳进行的母亲给药途径可能对新生儿更安全。在我们的研究中,早期和直接给予益生菌组合鼠李糖乳杆菌 GG 与双歧杆菌乳双歧杆菌 Bb-12 增加了 7 天时早产儿肠道中双歧杆菌的比例,但母亲给药途径的效果不如前者。