Inagaki Ryo, Inoue Akihiro, Miyazaki Yukihiro, Kanehisa Kota, Kunihiro Joji, Kondo Takuya, Katayama Eiji, Taniwaki Mashio, Shigekawa Seiji, Watanabe Hideaki, Kitazawa Riko, Kunieda Takeharu
Department of Neurosurgery, Ehime University School of Medicine, Toon, Japan.
Department of Hematology, Clinical Immunology and Infectious Diseases, Ehime University School of Medicine, Toon, Japan.
Surg Neurol Int. 2023 Mar 17;14:89. doi: 10.25259/SNI_1175_2022. eCollection 2023.
Intravascular large B-cell lymphoma (IVLBCL) is a rare entity among large B-cell non-Hodgkin lymphomas and is often difficult to diagnose. We report the case of a patient with IVLBCL who presented with central nervous system (CNS) symptoms alone, in which positron emission tomography (PET) enabled a rapid and accurate diagnosis.
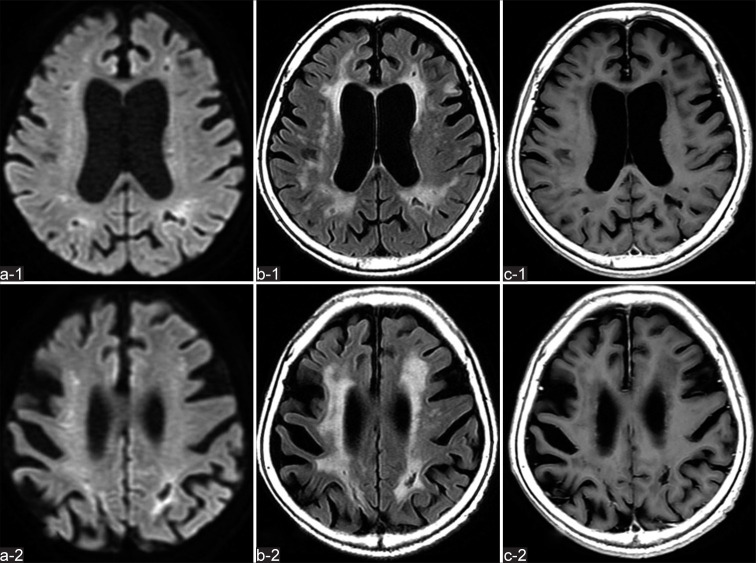
An 81-year-old woman was admitted to our hospital with a 3-month history of gradually progressive dementia and declining spontaneity. Magnetic resonance imaging revealed multiple hyperintense lesions bilaterally on diffusion-weighted imaging without enhancement on gadolinium-enhanced T1-weighted imaging. Laboratory findings showed elevated serum lactate dehydrogenase (626 U/L) and soluble interleukin-2 receptor (sIL-2R) (4692 U/mL). Cerebrospinal fluid (CSF) analysis showed slightly elevated levels of protein (166 mg/dL) and lymphocytic cells (29/μL), and β2-microglobulin (β2-MG) (4.6 mg/L) was highly elevated. Whole-body computed tomography revealed faint ground-glass opacities in the upper and middle lung fields and diffuse enlargement of both kidneys without lymph node swelling. F-fluorodeoxyglucose (FDG)-PET showed diffuse and remarkably high FDG uptake in both upper lungs and kidneys without uptake by lymph nodes, suggesting a malignant hematological disease. IVLBCL was confirmed histologically by incisional random skin biopsy from the abdomen. Chemotherapy using R-CHOP regimen in combination with intrathecal methotrexate injection was started on day 5 after admission and follow-up neuroimaging showed no signs of recurrence.
IVLBCL presenting with CNS symptoms alone is rare and often has a poor prognosis associated with delayed diagnosis, and various evaluations (including systemic analysis) are therefore necessary for early diagnosis. FDG-PET, in addition to identification of clinical symptoms and evaluation of serum sIL-2R and CSF β2-MG, enables rapid therapeutic intervention in IVLBCL presenting with CNS symptoms.
血管内大B细胞淋巴瘤(IVLBCL)在大B细胞非霍奇金淋巴瘤中是一种罕见的疾病,且常常难以诊断。我们报告了一例仅表现为中枢神经系统(CNS)症状的IVLBCL患者,正电子发射断层扫描(PET)实现了快速准确的诊断。
一名81岁女性因3个月来逐渐进展的痴呆和自发性减退入住我院。磁共振成像显示双侧扩散加权成像上有多个高信号病变,钆增强T1加权成像上无强化。实验室检查结果显示血清乳酸脱氢酶(626 U/L)和可溶性白细胞介素-2受体(sIL-2R)(4692 U/mL)升高。脑脊液(CSF)分析显示蛋白(166 mg/dL)和淋巴细胞(29/μL)水平略有升高,β2-微球蛋白(β2-MG)(4.6 mg/L)显著升高。全身计算机断层扫描显示上、中肺野有模糊的磨玻璃影,双肾弥漫性增大,无淋巴结肿大。氟脱氧葡萄糖(FDG)-PET显示双上肺和双肾有弥漫性且显著的FDG摄取,淋巴结无摄取,提示恶性血液病。通过腹部切口随机皮肤活检组织学确诊为IVLBCL。入院后第5天开始使用R-CHOP方案联合鞘内注射甲氨蝶呤进行化疗,后续神经影像学检查未显示复发迹象。
仅表现为CNS症状的IVLBCL很罕见,且常因诊断延迟而预后不良,因此早期诊断需要进行各种评估(包括全身分析)。除了识别临床症状以及评估血清sIL-2R和CSF β2-MG外,FDG-PET还能对表现为CNS症状的IVLBCL进行快速治疗干预。