Pompili Enrico, Baldassarre Maurizio, Zaccherini Giacomo, Tufoni Manuel, Iannone Giulia, Pratelli Dario, Palmese Francesco, Vizioli Luca, Faggiano Chiara, Bedogni Giorgio, Domenicali Marco, Caraceni Paolo
Department of Medical and Surgical Sciences, Alma Mater Studiorum - University of Bologna, Bologna, Italy.
Centre for Applied Biomedical Research (CRBA), Alma Mater Studiorum - University of Bologna, Bologna, Italy.
JHEP Rep. 2023 Feb 11;5(5):100698. doi: 10.1016/j.jhepr.2023.100698. eCollection 2023 May.
BACKGROUND & AIMS: Patients with decompensated cirrhosis present frequent hospitalisations with a relevant clinical and socio-economic impact. This study aims to characterise unscheduled readmissions up to 1-year follow-up and identify predictors of 30-day readmission after an index hospitalisation for acute decompensation (AD).
We performed a secondary analysis of a prospectively collected cohort of patients admitted for AD. Laboratory and clinical data at admission and at discharge were collected. Timing and causes of unscheduled readmissions and mortality were recorded up to 1 year.
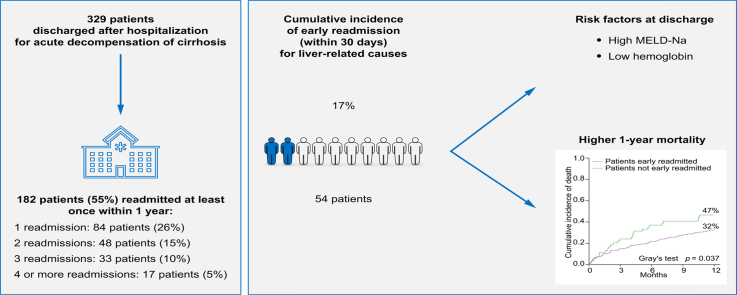
A total of 329 patients with AD were included in the analysis. Acute-on-chronic liver failure was diagnosed in 19% of patients at admission or developed in an additional 9% of patients during the index hospitalisation. During the 1-year follow-up, 182 patients (55%) were rehospitalised and 98 (30%) more than once. The most frequent causes of readmission were hepatic encephalopathy (36%), ascites (22%), and infection (21%). Cumulative incidence of readmission was 20% at 30 days, 39% at 90 days, and 63% at 1 year. Fifty-four patients were readmitted for emergent liver-related causes within 30 days. Early readmission was associated with a higher 1-year mortality (47 32%, = 0.037). Multivariable Cox regression analysis showed that haemoglobin (Hb) ≤8.7 g/dl (hazard ratio 2.63 [95% CI 1.38-5.02], = 0.003) and model for end-stage liver disease-sodium score (MELD-Na) >16 at discharge (hazard ratio 2.23 [95% CI 1.27-3.93], = 0.005), were independent predictors of early readmission. In patients with MELD-Na >16 at discharge, the presence of Hb ≤8.7 g/dl doubles the risk of early rehospitalisation (44% 22%, = 0.02).
Besides MELD-Na, a low Hb level (Hb ≤8.7 g/dl) at discharge emerged as a new risk factor for early readmission, contributing to identification of patients who require closer surveillance after discharge.
Patients with decompensated cirrhosis face frequent hospitalisations. In the present study, type and causes of readmissions were analysed during 1-year follow-up in patients discharged after the index hospitalisation for an acute decompensation of the disease. Early (30-day) liver-related readmission was associated with higher 1-year mortality. The model for end-stage liver disease-sodium score and low haemoglobin at discharge were identified as independent risk factors for early readmissions. Haemoglobin emerged as a new easy-to-use parameter associated with early readmission warranting further investigation.
失代偿期肝硬化患者频繁住院,具有显著的临床和社会经济影响。本研究旨在对长达1年随访期内的非计划再入院情况进行特征描述,并确定急性失代偿(AD)首次住院后30天再入院的预测因素。
我们对前瞻性收集的因AD入院患者队列进行了二次分析。收集了入院时和出院时的实验室及临床数据。记录了长达1年的非计划再入院时间和原因以及死亡率。
共有329例AD患者纳入分析。19%的患者入院时被诊断为慢加急性肝衰竭,另有9%的患者在首次住院期间发生慢加急性肝衰竭。在1年随访期内,182例患者(55%)再次住院,98例患者(30%)多次住院。再入院最常见的原因是肝性脑病(36%)、腹水(22%)和感染(21%)。30天时再入院的累积发生率为20%,90天时为39%,1年时为63%。54例患者在30天内因紧急肝脏相关原因再次入院。早期再入院与1年更高的死亡率相关(47%对32%,P = 0.037)。多变量Cox回归分析显示,血红蛋白(Hb)≤8.7 g/dl(风险比2.63[95%置信区间1.38 - 5.02],P = 0.003)和出院时终末期肝病-钠评分(MELD-Na)>16(风险比2.23[95%置信区间1.27 - 3.93],P = 0.005)是早期再入院的独立预测因素。在出院时MELD-Na >16的患者中,Hb≤8.7 g/dl使早期再次住院的风险加倍(44%对22%,P = 0.02)。
除了MELD-Na,出院时低Hb水平(Hb≤8.7 g/dl)成为早期再入院的新危险因素,有助于识别出院后需要更密切监测的患者。
失代偿期肝硬化患者面临频繁住院。在本研究中,对疾病急性失代偿首次住院后出院患者进行了1年随访,分析了再入院的类型和原因。早期(30天)肝脏相关再入院与更高的1年死亡率相关。终末期肝病-钠评分和出院时低血红蛋白被确定为早期再入院的独立危险因素。血红蛋白成为与早期再入院相关的新的易于使用的参数,值得进一步研究。