Wang Tongyu, Tan Wenting, Wang Xianbo, Zheng Xin, Huang Yan, Li Beiling, Meng Zhongji, Gao Yanhang, Qian Zhiping, Liu Feng, Lu Xiaobo, Yan Huadong, Zheng Yubao, Zhang Weituo, Yin Shan, Gu Wenyi, Zhang Yan, Dong Fuchen, Wei Jianyi, Deng Guohong, Xiang Xiaomei, Zhou Yi, Hou Yixin, Zhang Qun, Xiong Shue, Liu Jing, Long Liyuan, Chen Ruochan, Chen Jinjun, Jiang Xiuhua, Luo Sen, Chen Yuanyuan, Jiang Chang, Zhao Jinming, Ji Liujuan, Mei Xue, Li Jing, Li Tao, Zheng Rongjiong, Zhou Xinyi, Ren Haotang, Shi Yu, Li Hai
Department of Gastroenterology, Ren Ji Hospital, School of Medicine, Shanghai Jiao Tong University, Shanghai, China.
NHC Key Laboratory of Digestive Diseases (Renji Hospital, Shanghai Jiaotong University School of Medicine), China.
JHEP Rep. 2022 Jul 5;4(10):100529. doi: 10.1016/j.jhepr.2022.100529. eCollection 2022 Oct.
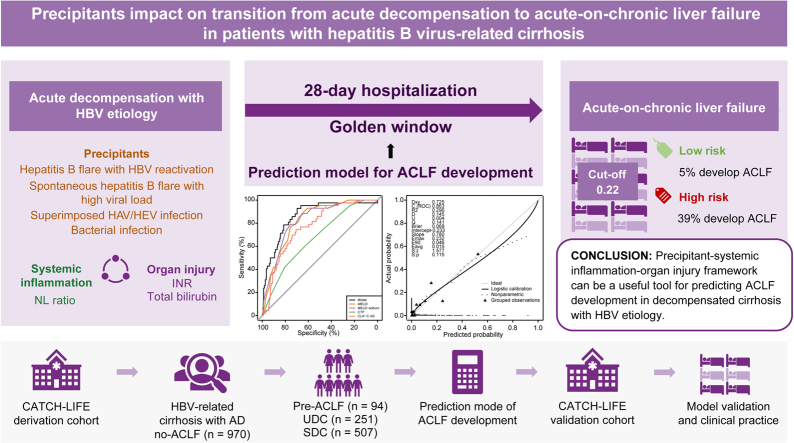
BACKGROUND & AIMS: Pre-acute-on-chronic liver failure (ACLF) is a distinct intermediate stage between acute decompensation (AD) and ACLF. However, identifying patients with pre-ACLF and predicting progression from AD to ACLF is difficult. This study aimed to identify pre-ACLF within 28 days, and to develop and validate a prediction model for ACLF in patients with HBV-related decompensated cirrhosis.
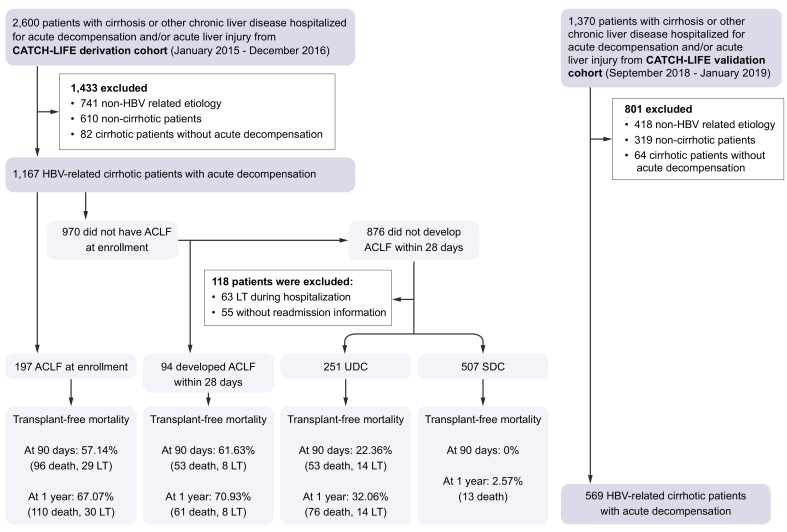
In total, 1,736 patients with HBV-related cirrhosis and AD were enrolled from 2 large-scale, multicenter, prospective cohorts. ACLF occurrence within 28 days, readmission, and 3-month and 1-year outcomes were collected.
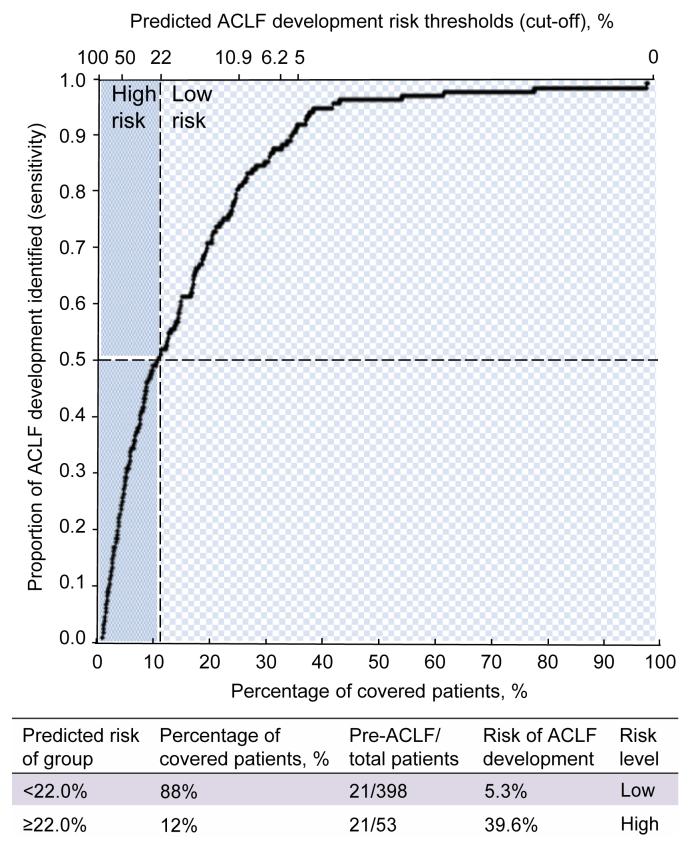
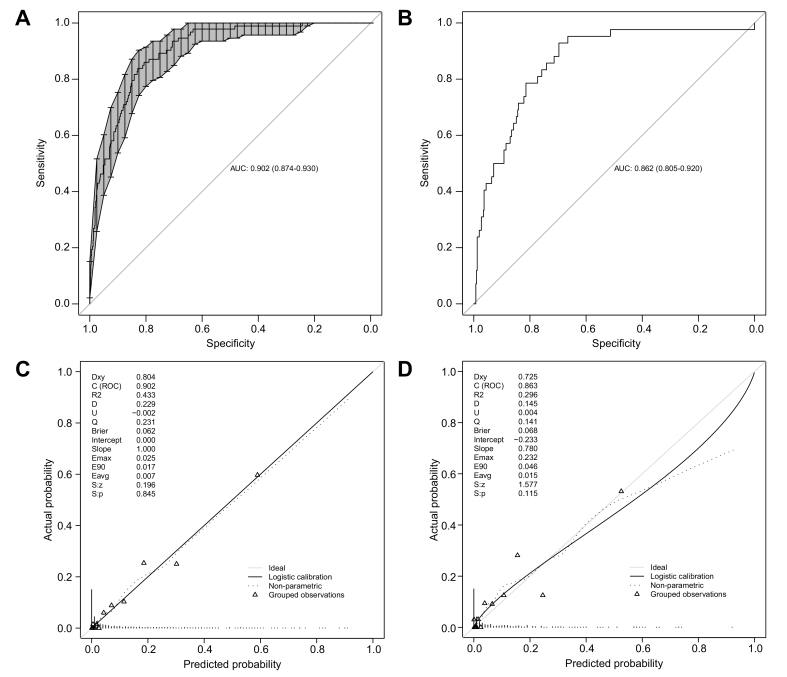
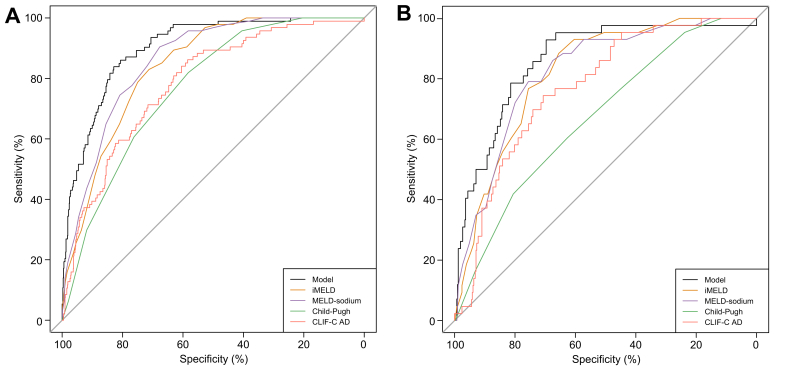
Among 970 patients with AD without ACLF in the derivation cohort, the 94 (9.6%) patients with pre-ACLF had the highest 3-month and 1-year LT-free mortality (61.6% and 70.9%, respectively), which was comparable to those with ACLF at enrollment (57.1% and 67.1%); the 251 (25.9%) patients with unstable decompensated cirrhosis had mortality rates of 22.4% and 32.1%, respectively; while the 507 (57.9%) patients with stable decompensated cirrhosis had the best outcomes (1-year mortality rate of 2.6%). Through Cox proportional hazard regression, specific precipitants, including hepatitis B flare with HBV reactivation, spontaneous hepatitis B flare with high viral load, superimposed infection on HBV, and bacterial infection, were identified to be significantly associated with ACLF occurrence in the derivation cohort. A model that incorporated precipitants, indicators of systemic inflammation and organ injuries reached a high C-index of 0.90 and 0.86 in derivation and validation cohorts, respectively. The optimal cut-off value (0.22) differentiated high-risk and low-risk patients, with a negative predictive value of 0.95.
Three distinct clinical courses of patients with AD are validated in the HBV-etiology population. The precipitants significantly impact on AD-ACLF transition. A model developed by the precipitant-systemic inflammation-organ injury framework could be a useful tool for predicting ACLF occurrence.
NCT02457637 and NCT03641872.
It was previously shown that patients with decompensated cirrhosis could be stratified into 3 groups based on their short-term clinical prognoses. Herein, we showed that this stratification applies to patients who develop cirrhosis as a result of hepatitis B virus infection. We also developed a precipitant-based model ( a model that incorporated information about the exact cause of decompensation) that could predict the likelihood of these patients developing a very severe liver disease called acute-on-chronic liver failure (or ACLF).
急性失代偿(AD)至慢加急性肝衰竭(ACLF)之间存在一个独特的中间阶段——前期慢加急性肝衰竭(pre-ACLF)。然而,识别pre-ACLF患者并预测AD向ACLF的进展较为困难。本研究旨在识别28天内的pre-ACLF,并建立和验证乙型肝炎病毒(HBV)相关失代偿期肝硬化患者发生ACLF的预测模型。
从2个大规模、多中心、前瞻性队列中纳入1736例HBV相关肝硬化和AD患者。收集28天内ACLF的发生情况、再次入院情况以及3个月和1年的结局。
在推导队列中970例无ACLF的AD患者中,94例(9.6%)pre-ACLF患者的3个月和1年无肝移植死亡率最高(分别为61.6%和70.9%),与入组时ACLF患者相当(分别为57.1%和67.1%);251例(25.9%)不稳定失代偿期肝硬化患者的死亡率分别为22.4%和32.1%;而507例(57.9%)稳定失代偿期肝硬化患者结局最佳(1年死亡率为2.6%)。通过Cox比例风险回归,在推导队列中确定了特定的促发因素,包括HBV再激活所致的乙型肝炎发作、高病毒载量的自发性乙型肝炎发作、HBV重叠感染和细菌感染,这些因素与ACLF的发生显著相关。一个纳入促发因素、全身炎症指标和器官损伤指标的模型在推导队列和验证队列中的C指数分别高达0.90和0.86。最佳截断值(0.22)区分了高风险和低风险患者,阴性预测值为0.95。
在HBV病因人群中验证了AD患者的三种不同临床病程。促发因素对AD-ACLF的转变有显著影响。由促发因素-全身炎症-器官损伤框架建立的模型可能是预测ACLF发生的有用工具。
NCT02457637和NCT03641872。
先前研究表明,失代偿期肝硬化患者可根据其短期临床预后分为3组。在此,我们表明这种分层适用于因乙型肝炎病毒感染而发生肝硬化的患者。我们还开发了一种基于促发因素的模型(一种纳入失代偿确切原因信息的模型),该模型可以预测这些患者发生一种称为慢加急性肝衰竭(ACLF)的非常严重肝病的可能性。