Division of Bone Diseases, Department of Medicine, Faculty of Medicine, Geneva University Hospitals, Rue Gabrielle-Perret-Gentil 4, 1205, Geneva 14, Switzerland.
Laboratory for Behavioural Neurology and Imaging of Cognition, Campus Biotech, University of Geneva, Geneva, Switzerland.
Aging Clin Exp Res. 2023 May;35(5):1015-1025. doi: 10.1007/s40520-023-02391-1. Epub 2023 Apr 8.
The European Working Group on Sarcopenia in Older People (EWGSOP2) recently revised its definition and diagnostic criteria for sarcopenia, placing muscle strength at the forefront. The pathogenesis of dynapenia (or low muscle strength) is still not fully understood, but there is emerging evidence that central neural factors constitute critical determinants.
Our cross-sectional study included 59 community-dwelling older women (mean age 73.1 ± 4.9 years). Participants underwent detailed skeletal muscle assessments for muscle strength defined by handgrip strength and chair rise time measurements using the recently published EWGSOP2 cut-off points. Functional magnetic resonance imaging (fMRI) was assessed during the performance of a cognitive dual-task paradigm, consisting of a baseline, two single-tasks (motor and arithmetic) and one dual-task (motor and arithmetic combined).
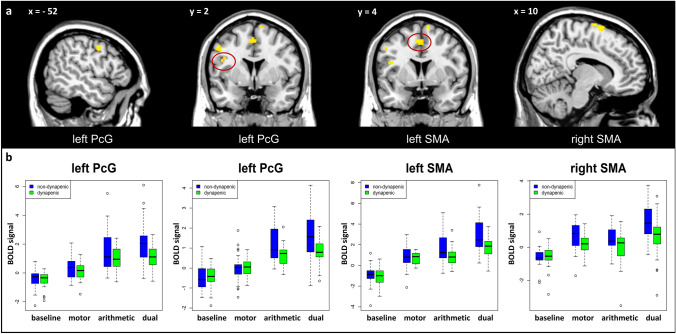
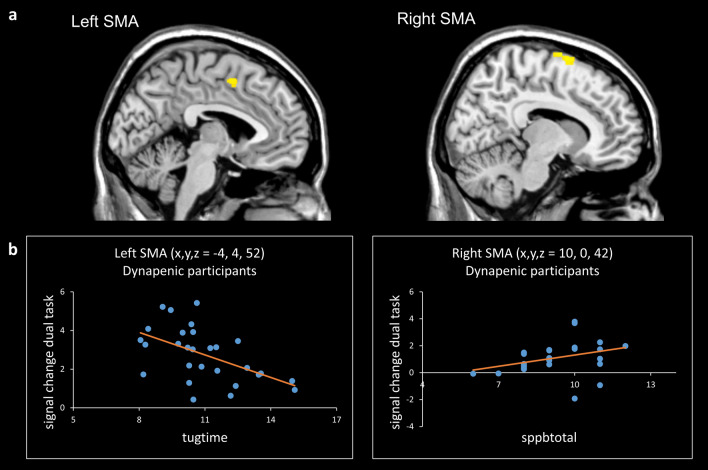
Forty-seven percent (28/59) of participants were classified as dynapenic. fMRI results revealed a differential recruitment of motor circuits in the brain during the dual-task condition in dynapenic as compared with non-dynapenic participants. In particular, while the brain activity during the single-tasks did not differ between the two groups, only during the dual-task non-dynapenic participants showed significant increased activation in dorsolateral prefrontal and premotor cortex, and in supplementary motor area as compared to dynapenic participants.
Our results point to a dysfunctional involvement of brain networks associated with motor control in dynapenia in a multi-tasking paradigm. A better knowledge of the link between dynapenia and brain functions could provide new impulses in the diagnosis and interventions for sarcopenia.
欧洲老年人肌肉减少症工作组(EWGSOP2)最近修订了其肌肉减少症的定义和诊断标准,将肌肉力量置于首位。动力性肌肉减少症(或低肌肉力量)的发病机制尚不完全清楚,但有新的证据表明,中枢神经因素构成了关键决定因素。
我们的横断面研究包括 59 名居住在社区的老年女性(平均年龄 73.1±4.9 岁)。参与者接受了详细的骨骼肌评估,肌肉力量通过握力和椅子起身时间测量来定义,使用最近发布的 EWGSOP2 截断值。在执行认知双重任务范式期间进行功能磁共振成像(fMRI)评估,该范式由基线、两个单任务(运动和算术)和一个双重任务(运动和算术组合)组成。
47%(28/59)的参与者被归类为动力性肌肉减少症。fMRI 结果显示,在双重任务条件下,动力性肌肉减少症患者的大脑运动回路的募集存在差异,与非动力性肌肉减少症患者相比。具体来说,虽然两组在单任务期间的大脑活动没有差异,但只有在双重任务期间,非动力性肌肉减少症患者的背外侧前额叶和运动前皮质以及辅助运动区的激活显著增加,与动力性肌肉减少症患者相比。
我们的结果表明,在多任务范式中,与运动控制相关的大脑网络在动力性肌肉减少症中存在功能障碍。更好地了解动力性肌肉减少症和大脑功能之间的联系,可以为肌肉减少症的诊断和干预提供新的思路。