Chung Kyung Bae, Hwang Ji-Hye, Kim Doyoung
Department of Dermatology and Cutaneous Biology Research Institute, Severance Hospital, Yonsei University College of Medicine, Seoul, Korea.
Ann Dermatol. 2023 Apr;35(2):140-145. doi: 10.5021/ad.20.341.
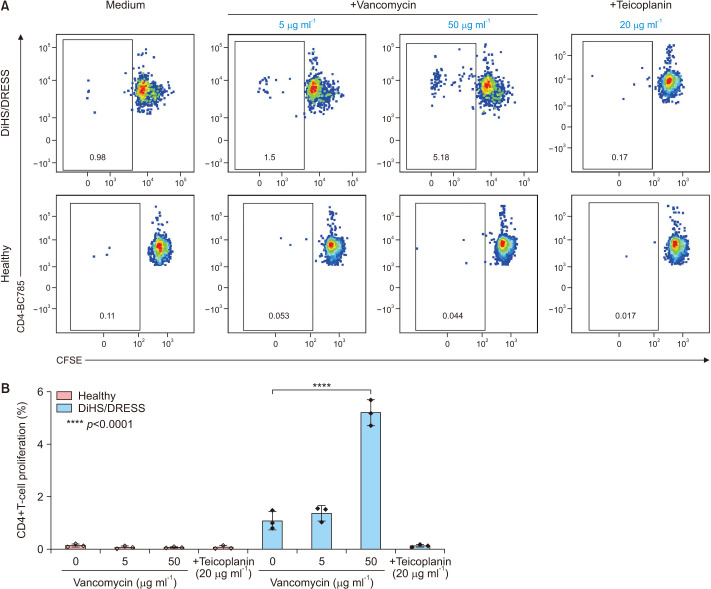
Drug-induced hypersensitivity syndrome (DiHS), also referred to as drug reaction with eosinophilia and systemic symptoms (DRESS), is a rare but potentially life-threatening condition induced by drug hypersensitivity that leads to significant morbidity and mortality and often occurs in patients undergoing combination antibiotic therapy. Due to a recent increase in the incidence of methicillin-resistant infections, the occurrence of vancomycin-induced DiHS/DRESS has increased rapidly. However, because of insufficient pharmacogenetic data on vancomycin-induced drug eruptions in Asians coupled with the risk of re-eliciting the symptoms by provocation tests, confirmation of the culprit drug in vancomycin-induced DiHS/DRESS is often challenging. Here, we report a case of vancomycin-induced DiHS/DRESS, where the causal relationship was confirmed using a lymphocyte transformation test (LTT). A 51-year-old woman was treated with combination antibiotics, including vancomycin, for infective pericarditis. The patient subsequently developed fever, facial edema, generalized rash followed by multiple internal organ involvement, including the kidney, lung, liver, and heart. Thus, based on the International Registry of Severe Cutaneous Adverse Reaction (RegiSCAR) criteria, the case was diagnosed as 'definite' DiHS/DRESS, although the culprit drug was obscured by combination antibiotic therapy. The LTT confirmed that vancomycin, but not other glycopeptide antibiotics, specifically induced T-cell proliferation in this case. Collectively, our case suggests that clinicians can utilize LTT to identify the causative medication of DiHS/DRESS when the clinical information is limited to defining the culprit drug.
药物性超敏反应综合征(DiHS),也称为伴有嗜酸性粒细胞增多和全身症状的药物反应(DRESS),是一种由药物超敏反应引起的罕见但可能危及生命的疾病,可导致严重的发病率和死亡率,且常发生于接受联合抗生素治疗的患者中。由于耐甲氧西林感染的发病率近期有所上升,万古霉素诱导的DiHS/DRESS的发生率迅速增加。然而,由于亚洲人万古霉素诱导的药疹的药物遗传学数据不足,加上激发试验有再次引发症状的风险,在万古霉素诱导的DiHS/DRESS中确定致病药物往往具有挑战性。在此,我们报告一例万古霉素诱导的DiHS/DRESS病例,其中通过淋巴细胞转化试验(LTT)证实了因果关系。一名51岁女性因感染性心包炎接受包括万古霉素在内的联合抗生素治疗。患者随后出现发热、面部水肿、全身性皮疹,随后多个内脏器官受累,包括肾脏、肺、肝脏和心脏。因此,根据国际严重皮肤不良反应登记处(RegiSCAR)标准,该病例被诊断为“确诊”DiHS/DRESS,尽管联合抗生素治疗掩盖了致病药物。LTT证实,在该病例中,是万古霉素而非其他糖肽类抗生素特异性诱导了T细胞增殖。总体而言,我们的病例表明,当临床信息有限难以确定致病药物时,临床医生可以利用LTT来识别DiHS/DRESS的致病药物。