Jain Ankit, Chen Chun-Chao, Chang Shih-Lin, Lin Yenn-Jiang, Lo Li-Wei, Hu Yu-Feng, Chung Fa-Po, Lin Chin-Yu, Chang Ting-Yung, Tuan Ta-Chuan, Chao Tze-Fan, Liao Jo-Nan, Liu Chih-Min, Wu Cheng-I, Chin Chye-Gen, Cheng Wen-Han, Liu Shin-Huei, Chou Ching-Yao, Lugtu Isaiah C, Chen Shih-Ann
Heart Rhythm Centre and Division of Cardiology, Department of Medicine, Taipei Veterans General Hospital, Taipei, Taiwan; Vardhman Mahavir, Medical College and Safdarjung Hospital, New Delhi, India.
Heart Rhythm Centre and Division of Cardiology, Department of Medicine, Taipei Veterans General Hospital, Taipei, Taiwan; Division of Cardiology, Department of Internal Medicine, Shuang Ho Hospital, Taipei Medical University, New Taipei City, Taiwan; Division of Cardiology, Department of Internal Medicine, School of Medicine, College of Medicine, Taipei Medical University, Taipei, Taiwan.
Indian Pacing Electrophysiol J. 2023 Jul-Aug;23(4):110-115. doi: 10.1016/j.ipej.2023.04.001. Epub 2023 Apr 11.
High-power short-duration (HPSD) and cryoballoon ablation (CBA) has been used for pulmonary vein isolation (PVI).
We aimed to compare the efficacy of PVI between CBA and HPSD ablation in patients with paroxysmal atrial fibrillation (PAF).
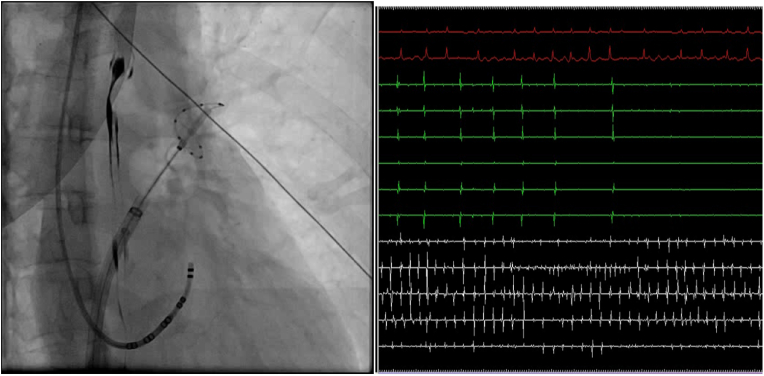
We retrospectively analyzed 251 consecutive PAF patients from January 2018 to July 2020. Of them, 124 patients (mean age 57.2 ± 10.1 year) received HPSD and 127 patients (mean age 59.6 ± 9.4 year) received CBA. In HPSD group, the radiofrequency energy was set as 50 W/10 s at anterior wall and 40 W/10 s at posterior wall. In CBA group, 28 mm s generation cryoballoon was used for PVI according the guidelines.
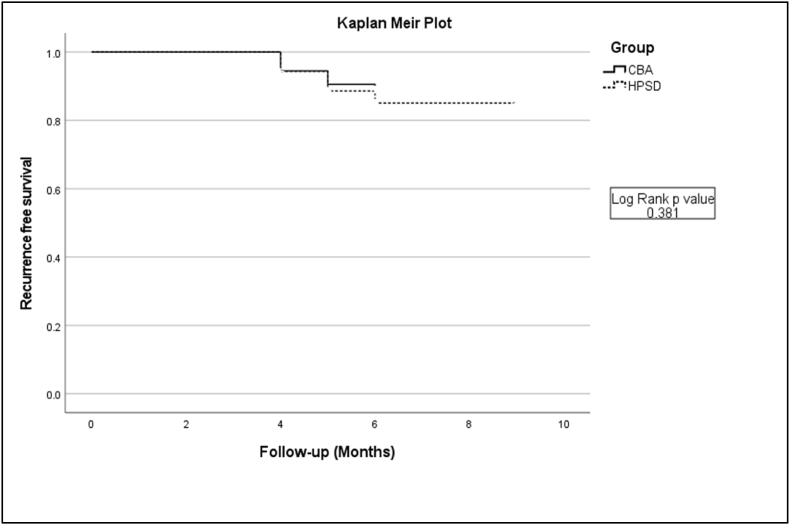
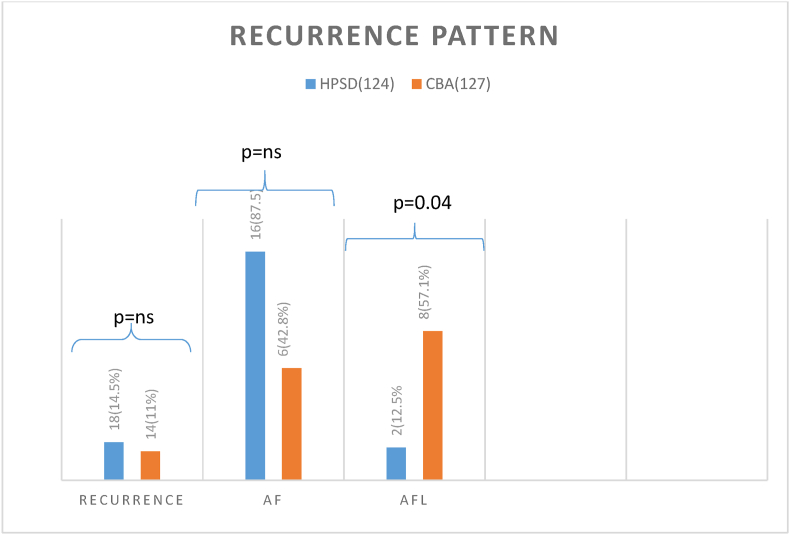
There was no significant difference in baseline characteristics between these 2 groups. The time to achieve PVI was significantly shorter in cryoballoon ablation group than in HPSD group (20.6 ± 1.7 min vs 51.8 ± 36.3, P = 0.001). The 6-month overall recurrence for atrial tachyarrhythmias was not significantly different between the two groups (HPSD:14.50% vs CBA:11.0%, P = 0.40). There were different types of recurrent atrial tachyarrhythmia between these 2 groups. Recurrence as atrial flutter was significantly more common in CBA group compared to HPSD group (57.1% vs 12.5%, P = 0.04).
In PAF patients, CBA and HPSD had a favourable and comparable outcome. The recurrence pattern was different between CBA and HPSD groups.
高功率短程(HPSD)和冷冻球囊消融(CBA)已用于肺静脉隔离(PVI)。
我们旨在比较阵发性心房颤动(PAF)患者中CBA和HPSD消融在PVI方面的疗效。
我们回顾性分析了2018年1月至2020年7月期间连续的251例PAF患者。其中,124例患者(平均年龄57.2±10.1岁)接受了HPSD,127例患者(平均年龄59.6±9.4岁)接受了CBA。在HPSD组中,前壁射频能量设置为50W/10秒,后壁为40W/10秒。在CBA组中,根据指南使用28mm第二代冷冻球囊进行PVI。
这两组患者的基线特征无显著差异。冷冻球囊消融组实现PVI的时间明显短于HPSD组(20.6±1.7分钟对51.8±36.3分钟,P = 0.001)。两组间6个月时房性快速心律失常的总体复发率无显著差异(HPSD:14.50%对CBA:11.0%,P = 0.40)。这两组间房性快速心律失常的复发类型不同。与HPSD组相比,CBA组心房扑动复发明显更常见(57.1%对12.5%,P = 0.04)。
在PAF患者中,CBA和HPSD具有良好且相当的疗效。CBA组和HPSD组的复发模式不同。