Hemostasis and Erythropathology Laboratory, Hematopathology, Pathology Department, Biomedical Diagnostic Center (CDB), Hospital Clínic de Barcelona, Universitat de Barcelona, Barcelona, Spain
Institut d'Investigacions Biomèdiques August Pi i Sunyer (IDIBAPS), Hospital Clínic de Barcelona, Barcelona, Spain.
J Immunother Cancer. 2023 Apr;11(4). doi: 10.1136/jitc-2022-006365.
Chimeric antigen receptor (CAR)-T cell-based immunotherapy constitutes a revolutionary advance for treatment of relapsed/refractory hematological malignancies. Nevertheless, cytokine release and immune effector cell-associated neurotoxicity syndromes are life-threatening toxicities in which the endothelium could be a pathophysiological substrate. Furthermore, differential diagnosis from sepsis, highly incident in these patients, is challenging. Suitable laboratory tools could be determinant for their appropriate management.
Sixty-two patients treated with CAR-T cell immunotherapy for hematological malignancies (n=46 with CD19-positive diseases, n=16 with multiple myeloma) were included. Plasma samples were obtained: before CAR-T cell infusion (baseline); after 24-48 hours; at suspicion of any toxicity onset and 24-48 hours after immunomodulatory treatment. Biomarkers of endothelial dysfunction (soluble vascular cell adhesion molecule 1 (sVCAM-1), soluble TNF receptor 1 (sTNFRI), thrombomodulin (TM), soluble suppression of tumorigenesis-2 factor (ST2), angiopoietin-2 (Ang-2)), innate immunity activation (neutrophil extracellular traps (NETs), soluble C5b-9 (sC5b-9)) and hemostasis/fibrinolysis (von Willebrand Factor antigen (VWF:Ag), ADAMTS-13 (A13), α2-antiplasmin (α2-AP), plasminogen activator inhibitor-1 antigen (PAI-1 Ag)) were measured and compared with those in cohorts of patients with sepsis and healthy donors.
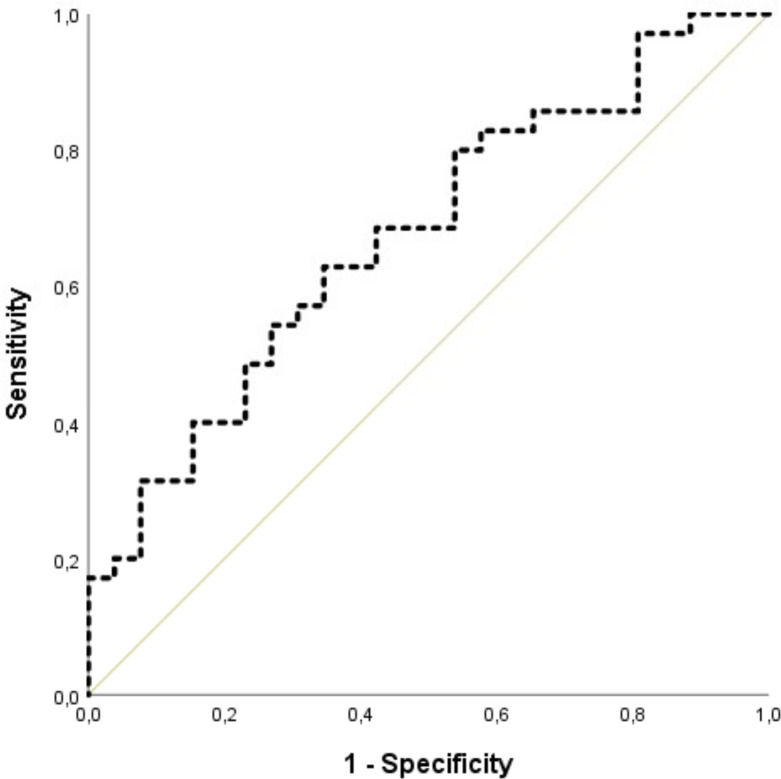
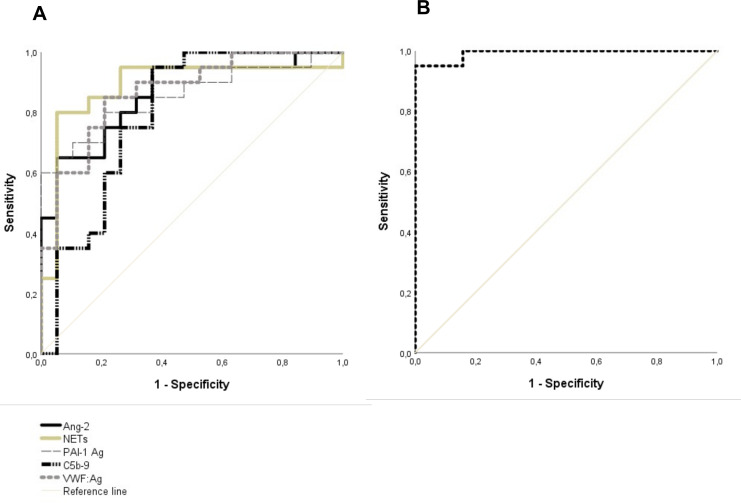
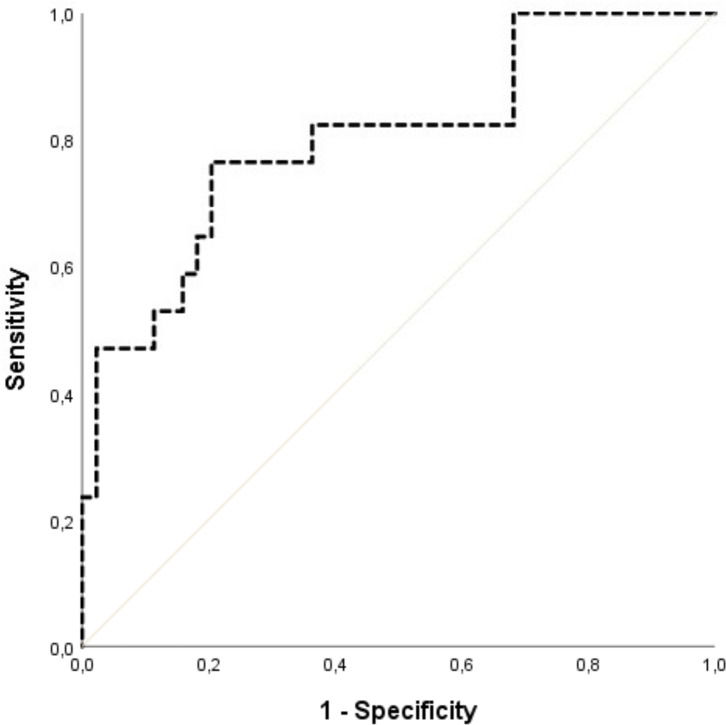
Patients who developed CAR-T cell toxicities presented increased levels of sVCAM-1, sTNFRI and ST2 at the clinical onset versus postinfusion values. Twenty-four hours after infusion, ST2 levels were good predictors of any CAR-T cell toxicity, and combination of ST2, Ang-2 and NETs differentiated patients requiring intensive care unit admission from those with milder clinical presentations. Association of Ang-2, NETs, sC5b-9, VWF:Ag and PAI-1 Ag showed excellent discrimination between severe CAR-T cell toxicities and sepsis.
This study provides relevant contributions to the current knowledge of the CAR-T cell toxicities pathophysiology. Markers of endotheliopathy, innate immunity activation and hemostatic imbalance appear as potential laboratory tools for their prediction, severity and differential diagnosis.
嵌合抗原受体 (CAR)-T 细胞免疫疗法为治疗复发/难治性血液系统恶性肿瘤带来了革命性的进步。然而,细胞因子释放和免疫效应细胞相关神经毒性综合征是危及生命的毒性,其中内皮细胞可能是一种病理生理底物。此外,与这些患者高度相关的败血症的鉴别诊断具有挑战性。合适的实验室工具可能对其适当管理具有决定性意义。
共纳入 62 例接受 CAR-T 细胞免疫疗法治疗血液系统恶性肿瘤的患者(CD19 阳性疾病 46 例,多发性骨髓瘤 16 例)。在以下时间点采集血浆样本:CAR-T 细胞输注前(基线);输注后 24-48 小时;怀疑任何毒性发生时以及免疫调节治疗后 24-48 小时。检测内皮功能障碍的生物标志物(可溶性血管细胞黏附分子 1(sVCAM-1)、可溶性肿瘤坏死因子受体 1(sTNFRI)、血栓调节蛋白(TM)、可溶性抑制肿瘤发生因子 2 因子(ST2)、血管生成素-2(Ang-2))、固有免疫激活(中性粒细胞细胞外陷阱(NETs)、可溶性 C5b-9(sC5b-9))和止血/纤溶(血管性血友病因子抗原(VWF:Ag)、ADAMTS-13(A13)、α2-抗纤溶酶(α2-AP)、纤溶酶原激活物抑制剂-1 抗原(PAI-1 Ag)),并与败血症患者和健康供者的这些标志物进行比较。
与输注后相比,发生 CAR-T 细胞毒性的患者在临床发病时 sVCAM-1、sTNFRI 和 ST2 水平升高。输注后 24 小时,ST2 水平是任何 CAR-T 细胞毒性的良好预测指标,ST2、Ang-2 和 NETs 的联合检测可区分需要入住重症监护病房的患者与临床表现较轻的患者。Ang-2、NETs、sC5b-9、VWF:Ag 和 PAI-1 Ag 的联合检测可极好地区分严重的 CAR-T 细胞毒性与败血症。
本研究为当前 CAR-T 细胞毒性的病理生理学知识提供了重要贡献。内皮功能障碍标志物、固有免疫激活和止血失衡似乎是其预测、严重程度和鉴别诊断的潜在实验室工具。