Takatsuka Daiki, Yoshimura Akiyo, Sawaki Masataka, Hattori Masaya, Kotani Haruru, Kataoka Ayumi, Horisawa Nanae, Ozaki Yuri, Endo Yuka, Nozawa Kazuki, Iwata Hiroji
Department of Breast Oncology, Aichi Cancer Center Hospital, Nagoya, Japan.
J Breast Cancer. 2023 Apr;26(2):117-125. doi: 10.4048/jbc.2023.26.e13. Epub 2023 Mar 17.
Fine-needle aspiration cytology (FNAC) of axillary lymph nodes (AxLNs) is performed to diagnose nodal metastasis in patients with breast cancer. Although the sensitivity of ultrasound-guided FNAC for identifying AxLN metastasis is in the range of 36%-99%, whether sentinel lymph node biopsy (SLNB) should be performed for neoadjuvant chemotherapy (NAC) patients with negative FNAC results is uncertain. This study aimed to determine the role of FNAC before NAC in the evaluation and management of AxLN in early breast cancer patients.
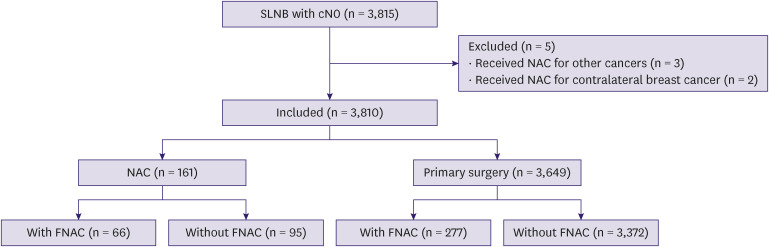
We retrospectively analyzed 3,810 clinically node-negative (a lymph node with no clinical metastasis without FNAC or radiological suspicion of metastasis with negative FNAC results) patients with breast cancer who underwent SLNB between 2008 and 2019. We compared the positivity rate of sentinel lymph nodes (SLNs) between patients who received and those who did not receive NAC with negative FNAC results or without FNAC and axillary recurrence rate in the neoadjuvant group with negative SLNB results.
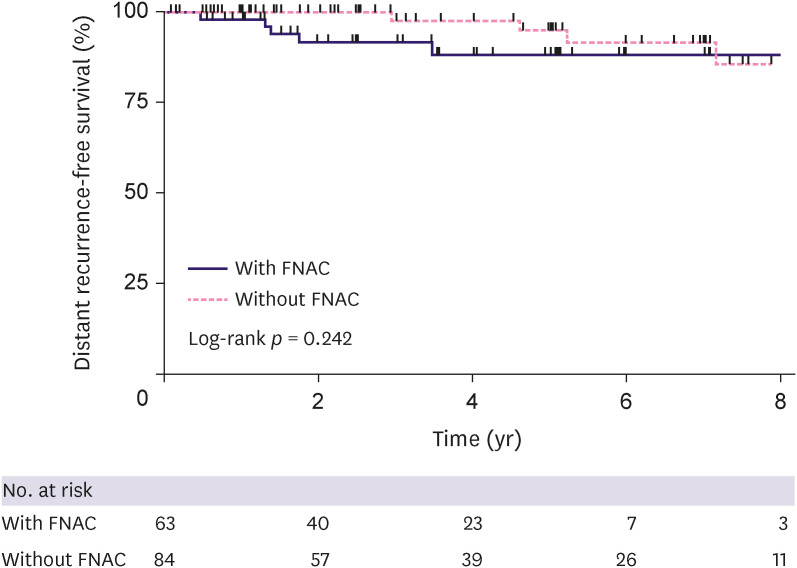
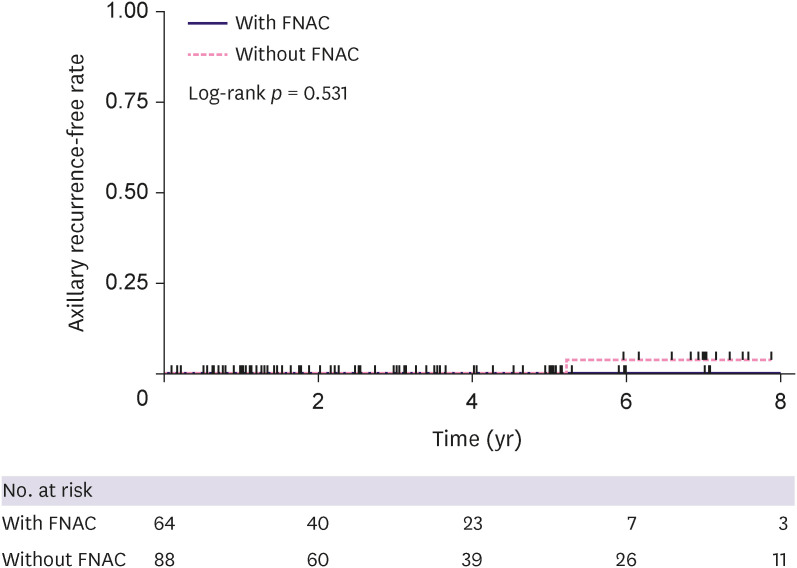
In the non-neoadjuvant (primary surgery) group, the positivity rate of SLNs in patients with negative FNAC results was higher than that in patients without FNAC (33.2% vs. 12.9%; < 0.001). However, the SLN positivity rate of patients with negative FNAC results (false-negative rate for FNAC) in the neoadjuvant group was lower than that in the primary surgery group (3.0% vs. 33.2%; < 0.001). After a median follow-up of 3 years, one axillary nodal recurrence was observed, which was a case from the neoadjuvant non-FNAC group. None of the patients in the neoadjuvant group with negative FNAC results had axillary recurrence.
The false-negative rate for FNAC in the primary surgery group was high; however, SLNB was the proper axillary staging procedure for NAC patients who have clinically suspicious AxLN metastases on radiologic examination but negative FNAC results.
对腋窝淋巴结(AxLNs)进行细针穿刺细胞学检查(FNAC)以诊断乳腺癌患者的淋巴结转移。尽管超声引导下FNAC识别AxLN转移的敏感性在36% - 99%范围内,但对于FNAC结果为阴性的新辅助化疗(NAC)患者是否应进行前哨淋巴结活检(SLNB)仍不确定。本研究旨在确定NAC前FNAC在早期乳腺癌患者AxLN评估和管理中的作用。
我们回顾性分析了2008年至2019年间接受SLNB的3810例临床淋巴结阴性(无临床转移的淋巴结,无FNAC或影像学怀疑转移且FNAC结果为阴性)的乳腺癌患者。我们比较了FNAC结果为阴性或未进行FNAC且接受和未接受NAC的患者之间前哨淋巴结(SLNs)的阳性率,以及新辅助组中SLNB结果为阴性的患者的腋窝复发率。
在非新辅助(初次手术)组中,FNAC结果为阴性的患者的SLNs阳性率高于未进行FNAC的患者(33.2%对12.9%;<0.001)。然而,新辅助组中FNAC结果为阴性的患者(FNAC假阴性率)的SLN阳性率低于初次手术组(3.0%对33.2%;<0.001)。中位随访3年后,观察到1例腋窝淋巴结复发,这是1例来自新辅助未进行FNAC组的病例。新辅助组中FNAC结果为阴性的患者均无腋窝复发。
初次手术组中FNAC的假阴性率较高;然而,对于影像学检查临床怀疑有AxLN转移但FNAC结果为阴性的NAC患者,SLNB是合适的腋窝分期程序。