Lucas Jean-Marc, Den Haese Jason P, Khatibshahidi Bianca Z, Storm Shawn W
Department of Osteopathic Medicine, 5000 Lakewood Ranch Blvd, Bradenton, Florida, USA.
Department of Orthopaedic Surgery, LECOM Health/Millcreek Community Hospital, Erie, Pennsylvania, USA.
J Orthop Case Rep. 2022 Dec;12(12):21-24. doi: 10.13107/jocr.2022.v12.i12.3448.
Altercations involving punching forces constitute 18.5% of all hand injuries. Intra-articular proximal phalanx base fractures of the index finger only account for 0.5% of all hand fractures. There is a paucity of ulnar claw deformities discussed in the literature, likely because ulnar neuropathies rarely remain untreated long enough to progress to deformity. We present the first reported case of a chronic ulnar claw deformity leading to an uncommon finger fracture pattern through an altered punching mechanism.
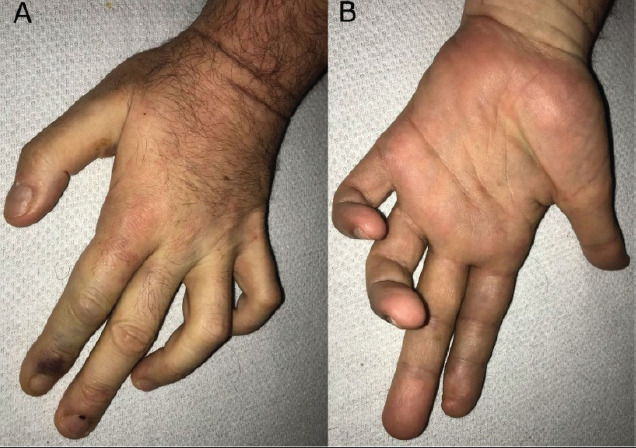
A 62-year-old right-hand dominant male who presented to the emergency department for a behavioral health examination was found to have an intra-articular fracture at the base of the proximal phalanx in the left index finger. This occurred secondary to an altered punching mechanism influenced by an existing ulnar claw deformity. Radiographs of the left hand revealed a simple, non-angulated, and minimally displaced oblique fracture at the base of the proximal phalanx. Diffuse edema and ecchymosis of the index finger and gross hypothenar, intrinsic, and adductor pollicis muscle atrophy were observed. A single source of ulnar clawing could not be elicited on the clinical examination alone. Management involving non-operative treatment with buddy-tape and non-weight bearing for 2 weeks was instituted. The patient did not follow-up with orthopedics for repeat evaluation.
This case demonstrates a unique fracture that likely occurred due to altered punching biomechanics from an ulnar claw deformity. The authors recommend that clinicians use their best judgment when comparing clinical findings to seemingly benign imaging studies. Early immobilization is crucial to prevent collapse and surgical intervention of intra-articular phalangeal fractures.
涉及拳击力的争吵导致的手部损伤占所有手部损伤的18.5%。食指近节指骨基底关节内骨折仅占所有手部骨折的0.5%。文献中关于尺侧爪形畸形的讨论很少,可能是因为尺神经病变很少长时间得不到治疗而发展为畸形。我们报告首例因慢性尺侧爪形畸形通过改变的拳击机制导致罕见手指骨折模式的病例。
一名62岁右利手男性因行为健康检查就诊于急诊科,发现左手食指近节指骨基底关节内骨折。这是由现有的尺侧爪形畸形影响的改变的拳击机制所致。左手X线片显示近节指骨基底简单、无成角且移位极小的斜形骨折。观察到食指弥漫性水肿和瘀斑以及小鱼际、固有肌和拇收肌明显萎缩。仅通过临床检查无法确定单一的尺侧爪形畸形来源。采取了用弹力胶带进行非手术治疗并2周不负重的处理措施。患者未到骨科进行复诊评估。
本病例显示了一种独特的骨折,可能是由于尺侧爪形畸形导致的拳击生物力学改变所致。作者建议临床医生在将临床发现与看似良性的影像学检查结果进行比较时要运用最佳判断力。早期固定对于防止关节内指骨骨折塌陷和手术干预至关重要。