Department of Surgery, University of California San Francisco, 550 16Th Street, 6Th Floor, San Francisco, CA, 94158, USA.
Helen Diller Family Comprehensive Cancer Center, San Francisco, CA, USA.
Int J Equity Health. 2023 Apr 14;22(1):68. doi: 10.1186/s12939-023-01883-w.
Colorectal cancer is a leading cause of morbidity and mortality across U.S. racial/ethnic groups. Existing studies often focus on a particular race/ethnicity or single domain within the care continuum. Granular exploration of disparities among different racial/ethnic groups across the entire colon cancer care continuum is needed. We aimed to characterize differences in colon cancer outcomes by race/ethnicity across each stage of the care continuum.
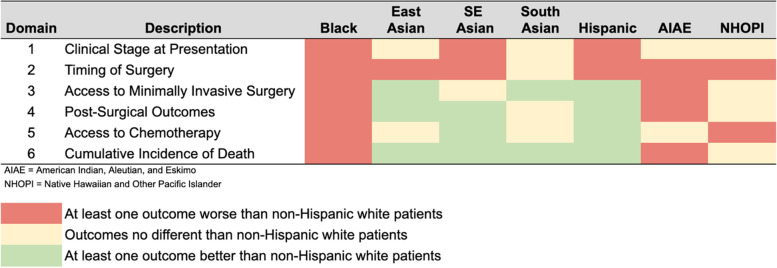
We used the 2010-2017 National Cancer Database to examine differences in outcomes by race/ethnicity across six domains: clinical stage at presentation; timing of surgery; access to minimally invasive surgery; post-operative outcomes; utilization of chemotherapy; and cumulative incidence of death. Analysis was via multivariable logistic or median regression, with select demographics, hospital factors, and treatment details as covariates.
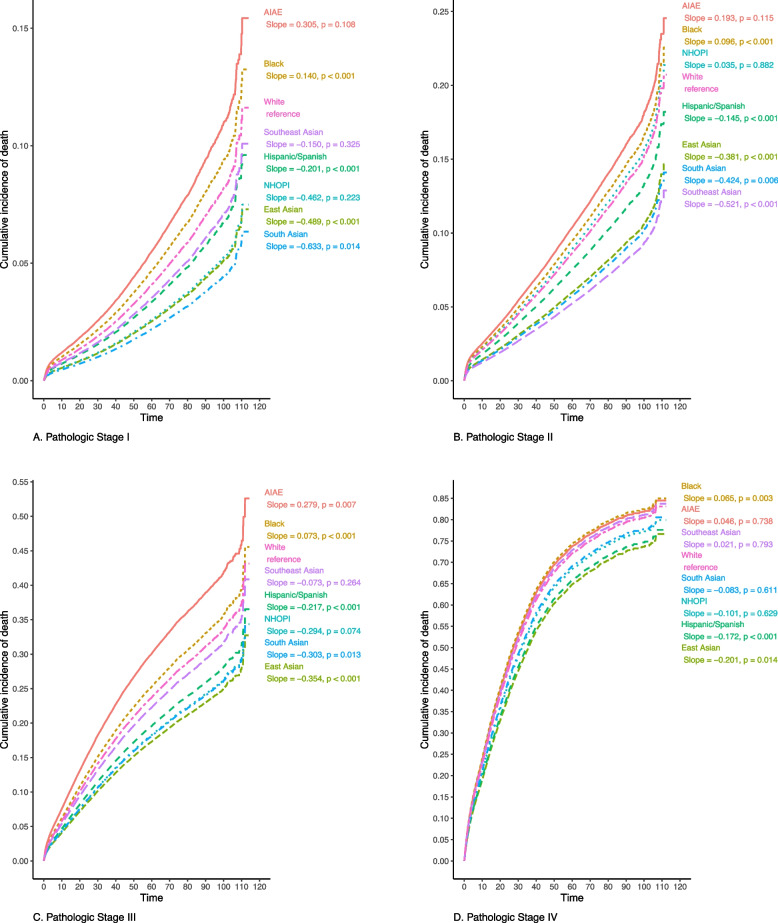
326,003 patients (49.6% female, 24.0% non-White, including 12.7% Black, 6.1% Hispanic/Spanish, 1.3% East Asian, 0.9% Southeast Asian, 0.4% South Asian, 0.3% AIAE, and 0.2% NHOPI) met inclusion criteria. Relative to non-Hispanic White patients: Southeast Asian (OR 1.39, p < 0.01), Hispanic/Spanish (OR 1.11 p < 0.01), and Black (OR 1.09, p < 0.01) patients had increased odds of presenting with advanced clinical stage. Southeast Asian (OR 1.37, p < 0.01), East Asian (OR 1.27, p = 0.05), Hispanic/Spanish (OR 1.05 p = 0.02), and Black (OR 1.05, p < 0.01) patients had increased odds of advanced pathologic stage. Black patients had increased odds of experiencing a surgical delay (OR 1.33, p < 0.01); receiving non-robotic surgery (OR 1.12, p < 0.01); having post-surgical complications (OR 1.29, p < 0.01); initiating chemotherapy more than 90 days post-surgery (OR 1.24, p < 0.01); and omitting chemotherapy altogether (OR 1.12, p = 0.05). Black patients had significantly higher cumulative incidence of death at every pathologic stage relative to non-Hispanic White patients when adjusting for non-modifiable patient factors (p < 0.05, all stages), but these differences were no longer statistically significant when also adjusting for modifiable factors such as insurance status and income.
Non-White patients disproportionately experience advanced stage at presentation. Disparities for Black patients are seen across the entire colon cancer care continuum. Targeted interventions may be appropriate for some groups; however, major system-level transformation is needed to address disparities experienced by Black patients.
结直肠癌是美国不同种族/族裔人群发病率和死亡率的主要原因。现有研究通常侧重于特定的种族/族裔或护理连续体中的单一领域。需要深入研究不同种族/族裔群体在整个结肠癌护理连续体中的差异。我们旨在通过种族/族裔来描述护理连续体各个阶段的结肠癌结局差异。
我们使用 2010-2017 年国家癌症数据库,通过六个领域检查了种族/族裔之间的结果差异:就诊时的临床分期;手术时机;微创手术的获得;术后结果;化疗的使用;以及死亡的累积发生率。分析通过多变量逻辑或中位数回归进行,选择了人口统计学、医院因素和治疗细节作为协变量。
符合纳入标准的患者共 326003 名(女性占 49.6%,非白人占 24.0%,包括黑人 12.7%、西班牙裔/拉丁裔 6.1%、东亚裔 1.3%、东南亚裔 0.9%、南亚裔 0.4%、美洲原住民/阿拉斯加原住民 0.3%、以及夏威夷原住民/其他太平洋岛民 0.2%)。与非西班牙裔白人患者相比:东南亚裔(OR 1.39,p<0.01)、西班牙裔/拉丁裔(OR 1.11,p<0.01)和黑人(OR 1.09,p<0.01)患者具有更高的晚期临床分期可能性。东南亚裔(OR 1.37,p<0.01)、东亚裔(OR 1.27,p=0.05)、西班牙裔/拉丁裔(OR 1.05,p=0.02)和黑人(OR 1.05,p<0.01)患者具有更高的晚期病理分期可能性。黑人患者经历手术延迟的可能性增加(OR 1.33,p<0.01);接受非机器人手术(OR 1.12,p<0.01);术后出现并发症(OR 1.29,p<0.01);术后 90 天以上开始化疗(OR 1.24,p<0.01);以及完全省略化疗(OR 1.12,p=0.05)。在调整不可改变的患者因素后(所有分期,p<0.05),黑人患者在每个病理分期的累积死亡率都显著高于非西班牙裔白人患者,但在调整可改变因素(如保险状况和收入)后,这些差异不再具有统计学意义。
非白人患者在就诊时不成比例地出现晚期。黑人患者在整个结肠癌护理连续体中都存在差异。针对某些群体可能需要采取有针对性的干预措施,但需要进行重大的系统级转变,以解决黑人患者所经历的差异。